




Contents
Scroll to:
https://doi.org/10.24060/2076-3093-2021-11-2-144-148
Scroll to:
Introduction. Neuroendocrine breast tumors represent a rare subtype of breast cancer, accounting for less than 1 % of all neuroendocrine neoplasms. Starting from their pathology definition, and going through their prevalence, prognosis and treatment, our knowledge is still really uncertain.
Materials and methods. The article presents a rare clinical observation of a neuroendocrine breast tumor. A breast fibroadenoma was diagnosed at the initial diagnosis stage in a private clinic; after a surgical treatment and further morphological study, it was estimated: a diagnosis of Cancer in situ of the left breast T1N0M0, stage I. Next, 3D-conformal remote radiation therapy was performed on the area of the left breast.
Results and discussion. After conducting positron emission tomography, multiple metastases were detected in the lymph nodes, bones, and liver. Additionally, micropreparations were consulted at the Federal Reference Center in St. Petersburg and at an independent third-party molecular biological laboratory in Germany (Munich). Given all the instrumental, molecular biological, histological and immunohistochemical studies of the patient, an individual regimen of drug therapy was selected.
Conclusion. After 18 months of personalized drug therapy, we observed a positive trend and a significant decrease in metabolic activity according to positron emission tomography.
Gantsev Sh.Kh., Schaller G., Gantsev K.Sh., Plikhta A.N., Kzyrgalin Sh.R., Rustamkhanov R.A. Neuroendocrine Breast Cancer. Clinical Observation. Personalized Approach. Creative surgery and oncology. 2021;11(2):144-148. https://doi.org/10.24060/2076-3093-2021-11-2-144-148
Neuroendocrine neoplasms (NENs) are a group of heterogeneous tumors deriving from neuroendocrine cells. Neuroendocrine cells are scattered around the body. Therefore, NENs have been reported to arise in multiple sites, such as central nervous system, respiratory tract, larynx, gastrointestinal tract, thyroid, skin, breast, and urogenital system [1].
Neuroendocrine breast tumors represent a rare subtype of breast cancer, accounting for less than 1 % of all neuroendocrine neoplasms. Starting from their pathology definition, and going through their prevalence, prognosis and treatment, our knowledge is still really uncertain [2].
The morphological diagnosis of breast NET is a problem not only for novice pathomorphologists, but even for experts. On the whole, the clinical significance and prognosis of such rare forms of breast cancer as NET, mucous (mucinous) carcinomas are still studied insufficiently. Most often, primary NETs are localized in the bronchopulmonary system, gastrointestinal tract and pancreas, originating from neuroendocrine cells of the corresponding organs. The NET of these localizations are well studied and best classified [3].
Primary neuroendocrine neoplasms of the breast (BNEN) are particularly rare, accounting for less than 1 % of NENs. Furthermore, the definition of BNEN is still quite confused [4].
In the 2003 World Health Organization (WHO) Pathology and Genetics of Tumours of the Breast and Female Genital Organs, BNEN were recognized as a distinct entity requiring — as diagnostic criteria — the expression of NE markers (specifically chromogranin and synaptophysin) in more than 50 % of cells [5–7]. It was later revised and the term changed into carcinomas with NE features in the 2012 WHO Classification of Tumours of the Breast [8]. World Health Organization Classification of Tumours, with the 50 % threshold for NE marker positivity considered arbitrary and therefore removed. In the more recent WHO classification published in 2019, BNEN can only be identified only when the proportion of neuroendocrine cells in samples is greater than 90 % [9].
BNEN are overall heterogeneous in their definition, being characterized by a various grade of differentiation and histological overlap, and at present, they do not identify a definite clinical entity, and no specific prognosis or therapy have been recognized yet [2].
At the present moment, the problem of diagnosing and treating NET in Russia is in the lack of statistical data on the morbidity and mortality caused by this pathology, the lack of doctors’ knowledge (oncologists, surgeons, endocrinologists, gastroenterologists) about the features of diagnosis, clinical course, principles of antitumor treatment and the lack of possibility or inaccessibility of IHC confirmation [10].
Clinical observation. Patient G., 33 years old, went to a private clinic (March 2018) to an oncologist with complaints on a lump in the left mammary gland. In the result of clinical examination, a rounded, smooth, easily displaced mass of up to 1.1 cm was revealed in the left mammary gland, at 9 o’clock, on the edge of the nipple halo. According to the ultrasound examination, a round formation with a diameter of about 11–12 mm was revealed. A puncture of the neoplasm was performed and a cytological conclusion was “breast fibroadenoma”. After the diagnosis of fibroadenoma of the left breast was established on an outpatient basis in a private clinic, a sectoral resection of the left breast was performed.
Macroscopic picture of the tumor: a roundish formation of gray-white color, up to 12 mm in size, a dense area of yellow-pink color without clear contours up to 3 mm was revealed in the section in the center of the tumor. Cytological examination of smears prints from a tumor section showed: fibroadenoma with malignancy, possibly lobular carcinoma in situ. Pathomorphological research showed: proliferating mastopathy, fibrosing adenosis; infiltrating ductal breast cancer of medium malignancy. IHC study ER++, TS = 6 (4 + 2), PR–, HER2–, Ki67 — 30 %. Conclusion: non-infiltrating ductal breast cancer in situ.
Postoperative diagnosis: Cancer in situ of the left breast T1N0M0, stage I. Further treatment was carried out in the Republican Clinical Oncology Center (Ufa). Considering the performed surgery, pathomorphological and IHC data, 3D conformal remote radiation therapy (RRT) was carried out, postoperative course, 5 days a week, on the Elekta Synergy apparatus on the left breast area, single PDD — 2,5 Gy, accumulated PDD — 45 Gy, 3 fields, bremsstrahlung energy of 6 MeV.
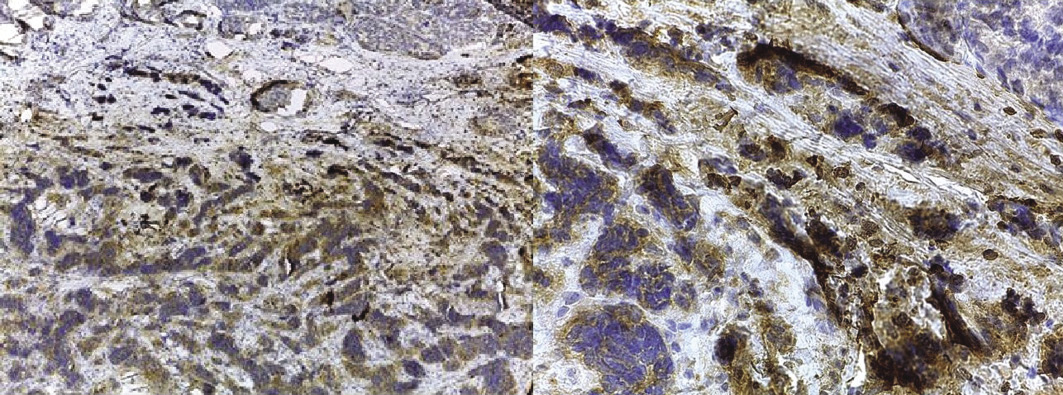
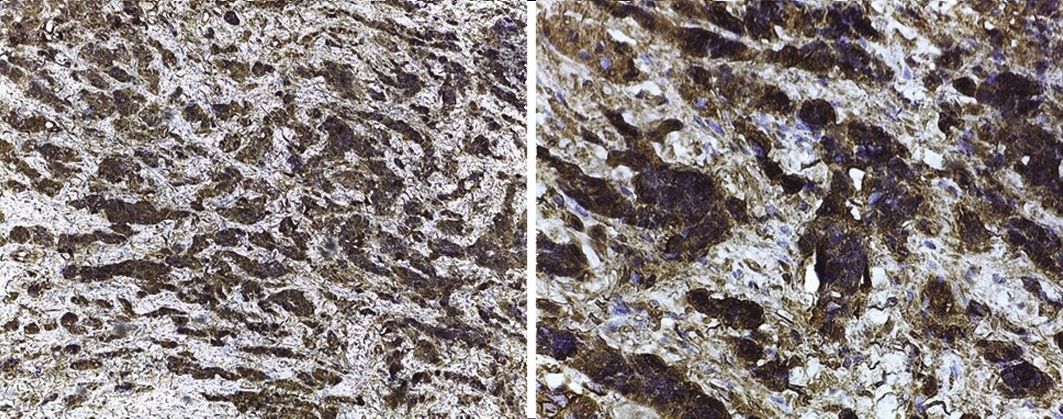
Additionally, micropreparations were consulted at the Federal Reference Center of St. Petersburg. Pathomorphological study showed that the tumor consists of small and medium cells, some of which are fusiform, with a pronounced crash phenomenon and pronounced mitotic activity. An IHC study showed a positive reaction in the tumor to synaptophysin and CgA; a granular reaction CKAE1/AE3 and a negative reaction in the tumor to CD56, p63, CK14, CD45 was noted. Positive reaction to estrogen receptors in 20 % of cells (5 points), negative reaction to progesterone receptors, HER2–, Ki67 — 70 %. Conclusion: “Neuroendocrine breast cancer, grade 3, Ki67 — 70 %, small cell variant”.
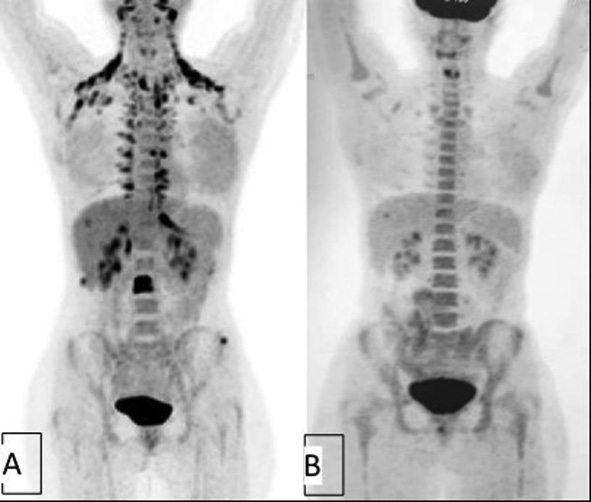
Taking into account that surgical removal of the tumor and radiation therapy were performed, it was decided to further monitor the patient. It should be noted that the patient complained of lumbar pain, sore throat when swallowing, and a number of other less significant complaints, therefore it was decided to perform positron emission tomography (PET). The study was carried out 4 months after the surgery. The PET conclusion: postoperative scar without foci of radiopharmaceuticals hyperfixation. Metabolically active metastases in the cervical (SUV max 6.3), supraclavicular (SUV max 9.7) and subclavian (SUV max 5.1) lymph nodes, bones (signs of osteolytic changes with pathological hyperfixation of the radiopharmaceuticals in the wing of the left iliac bone (SUV max 4.4), L3 body (SUV max 8.4), Th7 (SUV max 5.4)), liver (fig. 1A).
The results of skeletal scintigraphy are metastases in the Th7, L3 vertebrae, 2 rib on the front right, in the left ilium.
Micropreparations were additionally consulted and a new IHC study was conducted in an independent third-party molecular biological laboratory in Germany (Munich). The conclusion was received: the tumor tissue had vivid expression of estrogen receptors. In view of this, a combined hormone therapy was recommended. The essence of this treatment concept is to block estradiol receptors through the use of an aromatase inhibitor and the administration of estriol. The tumor cell division rate according to the study was 30 %, which dictated the need for cytostatic chemotherapy. The medication of choice in this case could be anthracyclines and/or gemcitabine and/or taxanes.
These preparations contain fibrosed stroma with mature cell ductal tissue at the edges. Intraductal proliferation of tumor cells with centered comedic necrosis is identified. In a number of zones, areas of strongly compressed cells are observed with suspicion for an atypical infiltrative glandular complex. Polarization — optically: dystrophic microcalcifications. Conclusion: “high degree ductal carcinoma in situ, with comedic necrosis and areas of invasive breast cancer NST G3 (non-specific type) with neuroendocrine differentiation”.
After all examinations and revisions of micropreparations, the Cancer in situ of the left breast [Tis (DCIS) N3M1] was diagnosed with metastases in the cervical, supraclavicular, subclavian lymph nodes, bones, liver stage 4.
Taking into consideration all the instrumental, molecular-biological, histological and IHC studies of the patient, an individual therapy regimen was selected. The combination of exemestane 25 mg per day with everolimus 10 mg/day (+ zoladex under the control of the level of FSH and estradiol). The toxicity of the combination with everolimus is usually higher in comparison to the standard chemotherapy regimen, but the patient experienced stopping of undesirable effects when the dose of everolimus was reduced.
The data of PET-CT of the whole body, 2 months after the beginning of personalized treatment, showed a positive trend. Metabolically subactive bone metastases were revealed: with pathological hyperfixation of radiopharmaceuticals in the wing of the left iliac bone (SUVmax 2.7), L3 body (SUVmax 2.9) (fig. 1B).
After 18 months of therapy, PET-CT showed no foci of radiopharmaceuticals hyperfixation; bone metastases with background activity, mainly with sclerosis in the wing of the left iliac bone, L3 body, TH7-no dynamics. Compared to the previous PET/CT — no negative dynamics. The patient continues her treatment. The pain stopped, the patient leads an active lifestyle.
Thus, the correct morphological diagnosis of breast NET can significantly expand the search for both personalized approaches and new therapeutic targets for the breast cancer treatment of [11].
Albeit BNEN were firstly described more than 40 years ago, and have been categorized more and more precisely thereafter, its rarity, together with still persisting diagnostic uncertainties, hampers drawing a precise clinical and prognostic picture. Furthermore, the lack of randomized controlled trials performed to compare different treatment strategies and their outcomes makes small case series the best available evidence on this issue, at present [12, 13].
In conclusion, it is likely that the cases diagnosed as primary BNEN are only minimally representative of their real prevalence. Only a systematic evaluation of neuroendocrine markers on all analyzed cases of breast cancer could give a reliable evaluation of the frequency of these tumors. Cancer registries centralizing uniform data collection, together with large multicentric studies, could sharpen our knowledge in the next future [3].
Shamil Kh. Gantsev — Dr. Sci. (Med.), Prof., Department of Oncology with Courses of Oncology and Pathological Anatomy for Advanced Professional Education
Ufa, Russian Federation
Gerhard Schaller — Prof., Dr. med
Munich, Germany
Kamil Sh. Gantsev — Dr. Sci. (Med.), Prof., Department of Oncology with Courses of Oncology and Pathological Anatomy for Advanced Professional Education
Ufa, Russian Federation
Andriy N. Plikhta — Prof., Dr. med
Eching, Germany
Shamil R. Kzyrgalin — Cand. Sci. (Med.), Assoc. Prof., Department of Oncology with Courses of Oncology and Pathological Anatomy for Advanced Professional Education
Ufa, Russian Federation
Rasul A. Rustamkhanov — Department of Oncology with Courses of Oncology and Pathological Anatomy for Advanced Professional Education
Ufa, Russian Federation
Gantsev Sh.Kh., Schaller G., Gantsev K.Sh., Plikhta A.N., Kzyrgalin Sh.R., Rustamkhanov R.A. Neuroendocrine Breast Cancer. Clinical Observation. Personalized Approach. Creative surgery and oncology. 2021;11(2):144-148. https://doi.org/10.24060/2076-3093-2021-11-2-144-148
Federal State Budgetary Educational Institution of Higher Education “Bashkir State Medical University” of the Ministry of Healthcare of the Russian Federation
96/98 Pushkin St., Ufa, 450008, Republic of Bashkortostan
Tel./fax: +7 (347) 273-56 -97
E-mail: csurgonco@bashgmu.ru






























