


ORIGINAL ARTICLES

Introduction. Cutaneous melanoma is an aggressive malignant tumor of neuroectodermal origin. According to statistics, most patients begin treatment at stages 2 and 3 of the disease. This worsens the prognosis and determines the need for expanding the scope of surgical treatment. Aim: To improve the outcomes of lymphatic surgery in patients with cutaneous melanoma. Materials and methods. A total of 190 medical records of cutaneous melanoma patients is analyzed. The feasibility of escalation and de-escalation of interventions is statistically assessed. The formed prospective sample includes 43 stage 3 patients subjected to surgery by intraoperative lymphorrhea-preventing methods. Results and discussion. Prophylactic lymphadenectomy appears nonoptimal since most patients have no evidence of lymph node involvement at the time of surgery. Refusal to perform an extended intervention scarcely ever meet the requirements of oncological safety. Of 43 patients with metastatic lymph node involvement, 25 persons had involvement of only one lymph node; two or more lymph nodes were involved in 18 patients. If lymphadenectomy is not performed, a high risk of recurrence is possible in 41% of patients. Patients with stage 1 cutaneous melanoma observe a low percentage of both lymph collector damage and regional metastasis in the distant period. Stage 3 patients have an increased risk of postoperative adverse events. Sealing of lymphatic vessels, careful treatment of surrounding structures, as well as the use of optical magnification show good results in the prevention of postoperative lymphorrhea to reduce the risk of other complications. Conclusion. The type of surgical intervention in patients with cutaneous melanoma should be based on prognose analysis, considered in accordance with possible risks and, if necessary, supplemented by the use of means to prevent complications.
Introduction. Patients with morbid obesity (BMI ≥ 35 kg/m²) are at high risk of developing postoperative ventral hernias due to increased intra-abdominal pressure, anatomical features and comorbidities. The main cause of hernias are postoperative complications, including seromas, hematomas, suppurations and eventrations, as well as factors increasing intra-abdominal pressure, such as cough, constipation, physical activity, etc. Aim. To reduce the incidence of postoperative ventral hernias and complications in patients with morbid obesity. Materials and methods. A method of endoprosthetics by laparotomy for preventing the formation of postoperative ventral hernias in high-risk patients has been developed and implemented into clinical practice. This method involves placing a synthetic implant (polypropylene) into the retromuscular space with fixation to the aponeurosis of internal oblique abdominal muscles. Results. The technical result of using this method involves the formation of a dense connective tissue scar and a reduction in the incidence of postoperative ventral hernias due to minimized risk of migration and rejection of the synthetic implant. Discussion. According to the presented data, the incidence of postoperative ventral hernias in the compared groups statistically significantly decreased from 30.7 to 5.2% (p = 0.039). The differences in the development of seromas and hematomas in the main and control groups are statistically insignificant (>0.05) amounting to 21.05 and 19.2%; seromas and hematomas recovered spontaneously without invasive interventions. Conclusion. For reducing the risk of postoperative ventral hernias, patients with morbid obesity are recommended to undergo preventive endoprosthetics during laparotomy surgery. The advantage of this method involves the reduction of postoperative complications, including the occurrence of chronic pain syndrome, and the improvement of the patients’ quality of life.
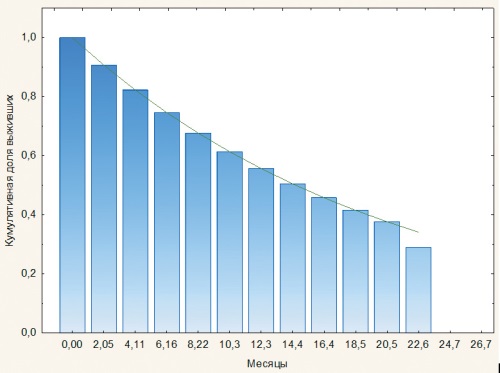
Introduction. Hepatocellular carcinoma is the third leading cause of cancer death worldwide with an extremely low five-year survival rate (20.3%) and colorectal cancer liver metastases accounting for significant 10–20% of all secondary tumors. Transarterial chemoembolization (TACE) represents a standard method of local palliative treatment; however, after the procedure, a stable hypoxic environment is formed contributing to aggressive relapses and further progression of the disease. The present study aims to assess the clinical efficacy and safety of TACE in patients with primary and metastatic liver cancer. Materials and methods. A retrospective analysis is conducted for 333 patients (181 men, 152 women) aged 19 to 83 years (mean age of 60.1 ± 0.55 years) treated at the National Medical Research Center for Oncology (Rostov-on-Don, Russian Federation). A total of 93 patients are diagnosed with hepatocellular carcinoma (ICD-10 C22.0); 240 have colorectal cancer metastases to the liver (ICD-10 C78.7). All underwent the TACE procedure. Two-year survival is analyzed using life tables, Kaplan-Meier method and Cox regression analysis to examine risk factors. Statistical analysis is performed using the Statistica 10 software. Results and discussion. During two years of observation, 61.9% of patients died; the overall survival rate is 38.1%. The highest risk of death was observed in the first two months after TACE, remaining high until the eighth month. A Kaplan-Meier analysis shows a significant reduction in survival after five months. Risk factors include disease stage, tumor morphology and patient gender: metastatic disease and male gender were associated with lower survival. Conclusion. Overall survival after TACE remains low, especially in the first months. The identified risk factors can be used for more accurate identification of high-risk groups to optimize combined therapy and develop more effective treatment strategies.
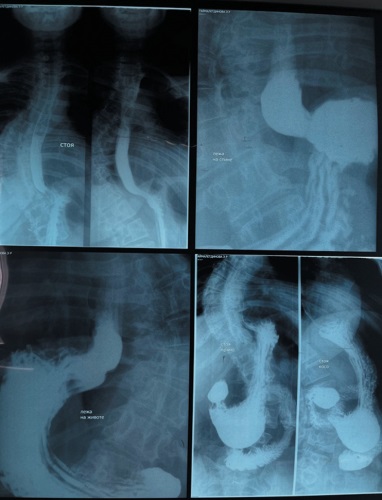
Introduction. A hiatal hernia (HH) is a condition of weakened diaphragmatic ligaments, resulting in stretching and enlargement of the hiatal opening and protrusion of abdominal organs into the pleural cavity. In the pathogenesis of HH, one of the leading roles is played by the structural degradation of connective tissue fibers of the esophageal-diaphragmatic membrane and weakening of the ligamentous apparatus of the stomach. A common method of HH surgical treatment involves laparoscopic Nissen fundoplication combined with anterior or posterior cruroraphy. An alternative method is the use of robot-assisted surgery. Materials and methods. During the period from April 2022 to January 2024, 113 robot-assisted laparoscopic fundoplications were performed in the thoracic surgery unit at the Hospital of Bashkir State Medical University (Ufa, Russian Federation). The patients were divided into two groups. A research group (n = 65) underwent robot-assisted laparoscopic Nissen fundoplication with modified cruroraphy and cuff fixation with Z-shaped sutures according to patent 2813330C1. A control group (n = 48) had standard laparoscopic Nissen fundoplication with anterior cruroraphy using interrupted sutures. The age of operated patients ranged from 35 to 65 years, including 72 and 28% of women and men, respectively. All surgical interventions were performed using the Da Vinci Si robotic system. Results and discussion. The use of an advanced technique (patent 2813330C1) in robot-assisted interventions for type III HHs prevents cuff migration and slippage, including into the pleural cavity, as well as the occurrence of the “telescope” symptom. It helps achieve symmetry and prevent cuff deformation and slippage, as well as ensures early patient activation and initiation of enteral nutrition through the use of laparoscopic techniques and Z-shaped suture with nonabsorbable suture material. Conclusion. The positive results of surgical interventions performed for type III HHs using the developed technique (patent 2813330C1) demonstrate the proposed method promising for videoendoscopic surgery.
Introduction. The implementation of ERAS protocol principles (Esophagectomy Complications Consensus Group) in thoracic surgery requires the provision of early enteral nutrition, including after Lewis esophagectomy. However, high incidence of esophagogastric anastomosis failure and postoperative encephalopathy hinders the safe use of sipping feeding, requiring improved methods for preventing these complications. Aim. To evaluate the effectiveness of implemented methods for preventing esophagogastric anastomosis failure and encephalopathy after Lewis esophagectomy. Materials and methods. A retrospective-prospective analysis of treatment results is conducted in 121 patients after Lewis esophagectomy. The main group (n = 35) underwent methods for preventing esophagogastric anastomosis failure and postoperative encephalopathy, protected by Russian patents No. 2791399 C1 and No. 2810178 C1. The control group (n = 86) consisted of patients operated using the standard technique. Results. The use of the proposed methods in the main group ensured a stable reduction in the incidence of anastomotic leakage (0 vs 4.7%, p < 0.05), including a statistically significant reduction in the overall incidence of postoperative complications (8.6 vs 17.4%, p < 0.05), hospital mortality (2.9 vs 12.8%, p < 0.05) and duration of hospitalization (16±3 vs 21±4 days, p < 0.05). The main group observed no signs of postoperative encephalopathy, impaired consciousness, cognitive functions, or laboratory test values associated with hyperammonemia. Discussion. The obtained data confirm the proposed prevention methods aiming at the key pathogenetic mechanisms for the development of complications including anastomotic failure and encephalopathy associated with portal hypertension. Elimination of biliary hypertension and intraoperative monitoring of anastomotic leakage ensure the safe implementation of sipping nutrition and reduce rehabilitation time. Conclusion. The use of the proposed methods for preventing anastomotic leakage and postoperative encephalopathy after Lewis esophagectomy ensures the integrity of sutures, prevention of metabolic and cognitive impairment in the early postoperative period, and safe implementation of sipping nutrition. The obtained results confirm the pathogenetic validity of the approach and substantiate the prospects for its further clinical application.
Introduction. Immediate breast reconstruction using smooth round implants has regained popularity following the abandonment of textured models due to their association with BIA-ALCL. However, the long-term results of DTI reconstruction with smooth implants remain poorly studied. The present study aims to evaluate the safety and efficiency of this method. Materials and methods. The retrospective study includes 48 patients (64 breasts) who underwent subcutaneous mastectomy with immediate reconstruction using smooth implants without additional covering materials. The observation period averages 54.5 months. The incidence of complications, oncological and surgical data, as well as risk factors for removal or replacement of implants are analyzed. Results. Early complications account for 10.94% with most common partial areola necrosis; late complications account for 20.31% mainly as type III–IV capsular contracture according to Baker. In 75% of cases, the implant was retained. High BMI, large implant volume and weight of removed tissue are significant factors in the development of complications. Discussion. The obtained data demonstrate comparable or better results compared to foreign studies. The absence of covering materials and subpectoral placement caused no negative effect on the incidence of infections; however, they correlate with animation deformity. The presence of postoperative radiation therapy significantly increases the risk of contracture. Conclusion. Immediate breast reconstruction using smooth implants demonstrates satisfactory long-term results with a low complication rate. The method can be considered as a safe alternative in conditions of limited access to ADM.
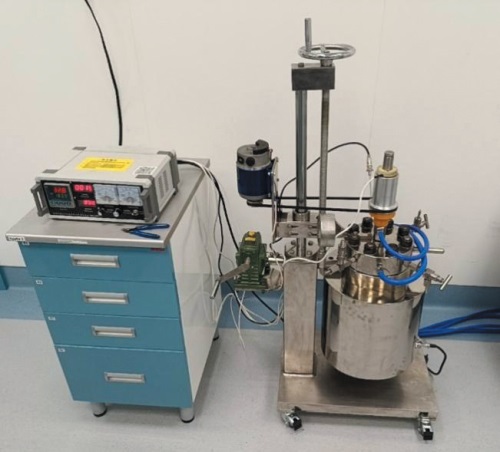
Introduction. Additive manufacturing of hydroxyapatite (HA) ceramics is considered a promising approach to creating personalized bone implants. However, highly loaded photopolymer suspensions assume precise composition and exposure conditions to ensure stable printing and product quality. The present study aims to develop a photopolymer suspension based on HA of in-house synthesis for the additive production of ceramic implants using DLP 3D printing. Materials and methods. HA is synthesized by coprecipitation and hydrothermal synthesis methods in aqueous solutions of calcium and phosphate salts. The powder is milled and fractionated for assessing the morphology and element composition using scanning electron microscopy and energy-dispersive X-ray fluorescence analysis, respectively. A photopolymer suspension with 60 wt. % of the inorganic phase, developed based on the synthesized HA, contains acrylate monomers, photoinitiating system and dispersing additives. In addition, photopolymerization is studied on a DLP 3D printer at different UV radiation powers and exposure times. Results and discussion. The synthesized well-crystallized HA has lamellar and nanostructured morphology, as well as developed porosity; the predominance of calcium and phosphorus without significant toxic impurities is confirmed. At a radiation power of 40 mW/cm², the optimal exposure time of 6–10 s ensures the formation of uniformly hardened layers with a thickness of about 0.7–0.9 mm and a thickness plateau at a further increase in exposure time. Conclusion. The obtained data indicate that the combination of controlled HA morphology and specially selected photopolymer matrix provides sufficient polymerization depth and layer stability required for DLP printing of complex geometries. High specific surface area and porosity of HA further enhance its potential in tissue engineering. The developed photopolymer suspension based on HA of in-house synthesis demonstrates suitability for DLP 3D printing and can be used as a basis for creating personalized ceramic implants in traumatology, orthopedics, neurosurgery, and maxillofacial surgery.
CLINICAL CASES
Introduction. Liver transplantation represents the definitive treatment for patients with end-stage liver disease. In liver transplant recipients, strictures of the biliary-digestive anastomosis and cholelithiasis of various localizations may occur. However, routine endoscopic procedures may be ineffective in some patients with complex forms of cholelithiasis and biliary strictures. In such situations, the SpyGlass DS™ direct digital cholangioscopy method is promising. Materials and methods. Clinical case: a 66-year-old patient in the late postoperative period after orthotopic related liver transplantation was diagnosed with a stricture of the reconstructive hepaticojejunostomy on the Roux-en-Y loop and intrahepatic cholelithiasis. The performed hybrid intervention includes: balloon dilation of the stricture and intrahepatic lithotripsy, lithoextraction using SpyGlass DS™ cholangioscopy, as well as percutaneous transhepatic drainage of the biliary tract under radiographic control. Results and discussion. Direct cholangioscopy ensured the safe elimination of hepatolithiasis and hepaticojejunostomy stricture in a patient after liver transplantation. External drainage with the possibility of delayed cholangiography was used to monitor the function of bile secretion with gradual replacement of drains. Conclusion. Direct digital cholangioscopy represents an important tool for the diagnosis and treatment of biliary complications in liver transplant recipients.
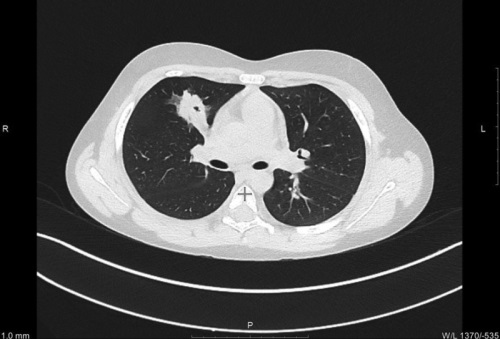
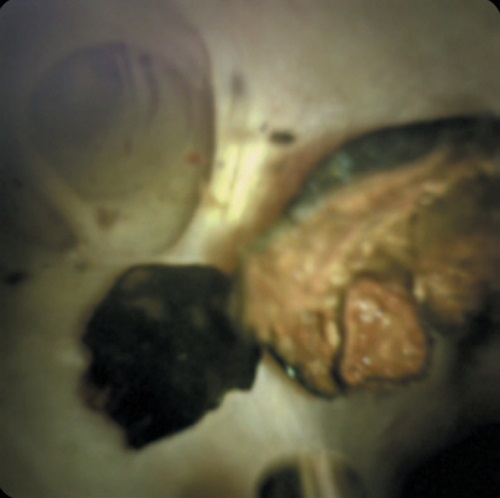
Introduction. Lung cancer in children is an extremely rare pathology occurring in less than 0.2 % of all childhood tumors. The most frequently detected tumors are adenocarcinoma and carcinoid tumors, which are often diagnosed at late stages due to the lack of specific symptoms and difficulties in differential diagnosis. Materials and methods. The article presents a clinical case of invasive mucinous adenocarcinoma of the lung in a 9-year-old child. Results. The tumor was incidentally found during a chest computed tomography scan. Changes in the lungs were assessed as destructive pneumonia, for which the patient received long-term treatment resulted in clinical improvement. However, a control computed tomography scan revealed negative dynamics. Given the localization of changes in one lobe, the patient underwent an upper lobectomy with systematic mediastinal lymph node dissection after preoperative preparation. Histologically, the diagnosis was invasive mucinous adenocarcinoma of the lung. No specific antitumor treatment was administered. The patient is currently under dynamic observation without signs of relapse. Discussion. This clinical case demonstrates the problems of diagnosing lung cancer in children, as well as the problems of staging the disease and determining treatment tactics. Conclusion. The performed study emphasizes the need to develop clear clinical guidelines for the diagnosis and treatment of lung cancer in children, taking into account anatomical and physiological characteristics of the child’s body.
REVIEWS
The present paper reviews contemporary scientific literature devoted to acute non-occlusive mesenteric ischemia (ANMI) as a severe pathology with a mortality rate of up to 80 %. The key aspects of pathogenesis, main risk factors and features of the clinical picture that complicate early diagnosis are considered. Particular attention is paid to the capabilities and limitations of contemporary diagnostic methods, including multislice computed tomography angiography (MSCT-A) and determination of biomarkers. Conservative treatment strategies, such as anticoagulant and systemic vasodilatation therapy, and surgical interventions, including revascularization, resection of non-viable sections of the intestine and damage control surgery tactics are analyzed in detail. The critical role of exploratory laparotomy and laparoscopy in verifying the diagnosis and intraoperative assessment of intestinal viability is discussed. The emphasis is put on the need for a multidisciplinary approach and creation of specialized centers to improve treatment outcomes.
Postoperative complications represent a pressing issue of clinical medicine, worsening the prognosis and increasing the risk of death in surgical patients, especially in abdominal and oncological surgery. According to contemporary concepts, microcirculatory dysfunction appears to be an important pathophysiological factor underlying tissue hypoperfusion and development of unfavorable postoperative outcomes. The present review summarizes current data on the relationship between microcirculation disorders both in the surgical area and body as a whole and postoperative complications of abdominal surgery. The review addresses the following issues: (1) epidemiology of postoperative complications and its relevance in clinical surgery and resuscitation; (2) pathophysiology of perioperative microcirculatory disorders, including hemorrhagic shock, disseminated intravascular coagulation (DIC) and endothelial dysfunction; (3) organ-specific changes in microcirculation in surgical diseases; (4) contemporary diagnostic and monitoring methods for tissue perfusion assessment; (5) prognostic and diagnostic value of a number of microcirculation parameters; (6) contemporary therapeutic approaches to tissue perfusion optimization and complication prevention. Understanding the important role of microcirculation in ensuring tissue perfusion and oxygenation justifies the use of intensive care methods focused on microcirculation and thus the prevention of organ ischemia, infectious and other postoperative complications.

The risk of developing postoperative complications directly depends on the biocompatibility of implant systems, which is largely determined by the condition and properties of their surface. Hydroxyapatite (HA) coatings are characterized by maximum similarity of structural and functional properties to those of bone tissue, which determines their wide application in biomedical engineering. Therefore, HA as a modifying surface coating can significantly increase the biocompatibility of implants and activate osseointegration processes. Today, thin HA coatings are mainly applied using thermal spraying methods at temperatures close to the melting point of the original material. However, exposure to high temperatures decreases the biocompatibility of the final coating and limits the introduction of heat-labile bioactive additives into its composition. In this regard, cold spraying technologies represent a promising direction, potentially superior to standard thermal methods. However, high brittleness of HA significantly complicates the low-temperature application of strong and uniform coatings. Thus, the selection of an optimal technological approach and establishment of rational spraying parameters represent key conditions for the formation of coatings with the required physicochemical characteristics increasing the efficiency of osseointegration. This paper presents a systematic analysis of experimental studies aimed at developing a conceptual framework for selecting powder, substrate and cold spraying parameters aimed at obtaining high-quality HA coatings with improved biomedical properties.

ISSN 2307-0501 (Online)





























