


ORIGINAL ARTICLES
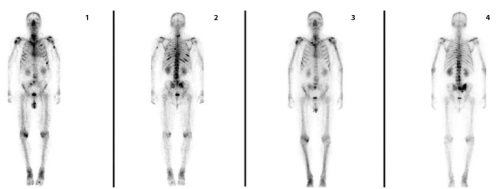
Introduction. Radionuclide therapy of bone metastases with radium-223 dichloride has been approved for patients with castration-resistant prostate cancer. Targeted therapy, which is being actively introduced into clinical practice, can improve overall survival rates, reduce pain with the possibility of discontinuing potent analgesic drugs, and reduce or delay the risk of potentially serious complications, such as pathological fractures and spinal cord compression. Objective. To evaluate the effectiveness of radium-223 dichloride in patients with castration-resistant prostate cancer. Materials and methods. Since 2023, at the Clinic of the Bashkir State Medical University, 43 patients with metastatic castrationresistant prostate cancer have received radionuclide therapy. Prior to each administration of radium-223 dichloride, blood parameters and prostate-specific antigen were monitored; functional status and pain syndrome were assessed. Patients were divided into groups depending on the use of radium-223 dichloride as a second-, third-, or fourth-line therapy. The drug effectiveness was assessed using control bone scintigraphy. Results and discussion. 62.7% of the patients who completed the course of radionuclide therapy showed stabilization of the process, which is consistent with the data of key publications of the largest world databases. Overall survival was higher in the group receiving the drug as a second-line therapy compared to that in the groups of later lines. During treatment, pain syndrome decreased in 58% of patients. In the general group, the alkaline phosphatase level decreased by 16.4%, which is consistent with the data of the ALSYMPCA phase 3 randomized study. Conclusion. Our study has confirmed the clinical effectiveness of radium-223 dichloride, thereby contributing to the evidence base for the optimization of its application in routine oncological practice. Since radium-223 dichloride is contraindicated in visceral metastases and is recommended as a second-line therapy, continuity in the work of specialists and timely routing of patients for early appointment are of high importance.

Introduction. Surgical staging is an essential component of breast cancer treatment. Sentinel lymph node biopsy (SLNB) can be used to exclude or confirm metastatic involvement of lymphatic collectors. Despite minimal invasiveness of this procedure, surgeons still encounter adverse events in the postoperative period. The aim of this study was to explore ways of reducing the risk of postoperative complications after minimally invasive interventions on the lymphatic system. Materials and methods. We analyzed the medical records of 114 patients who underwent SLNB. The incidence of post‑operative complications was assessed in patient groups stratified by the number of excised lymph nodes. Based on prior experience in managing lymphorrhea, a subgroup of 28 patients was formed, in whom SLNB was performed with optical magnification, a double coagulation technique, and gentle principles of electrosurgery. Results and discussion. Reducing the number of excised nodes decreased the likelihood of complications, including seroma formation. Dividing patients into subgroups according to the number of removed lymph nodes revealed cases of metastatic spread to more collectors than the method could resolve. Taking this into account, the issue of abandoning lymph node dissection in the presence of sentinel node metastasis necessitates excision of at least two lymph nodes, with three excised nodes being considered optimal. Surgical interventions performed in accordance with these principles and using the described techniques were associated with lower risks of complications. Conclusion. The development of new technical solutions in surgical practice is very promising in improving patients’ quality of life. However, de-escalation of surgical management must be consistent and safe; otherwise, all the advantages of a well-performed operation are negated by excessive oncological risk.
Introduction. The increase in surgical activity for diseases of the hepatopancreatobiliary system has also led to a higher frequency of postoperative complications. The development of postoperative intra-abdominal purulentseptic complications is one of the main causes of adverse outcomes, which necessitates the improvement of their management methods. The aim of this study was to analyze a large clinical dataset in order to evaluate the incidence and structure of intraabdominal purulent-septic complications after hepatopancreatobiliary surgery. Materials and methods. A large clinical dataset (4,292 cases) collected over five years was analyzed. The overall incidence of postoperative complications after hepatopancreatobiliary surgery was 4.7% (202 out of 4,292). Among these, purulent-septic complications accounted for 55.9%, or 2.63% of all procedures. Results. Among postoperative purulent-septic complications, the most common were suppurative cholangitis (23.0%), infected biliary leaks (19.5%), liver abscesses (15.9%) and perihepatic abscesses (14.2%). Less frequent were peritonitis (10.6%), abscesses of the omental bursa (8.8%), and incomplete intestinal fistulas (8.0%). Discussion. Advances in surgical technology, anesthetic and intensive care support, as well as improvements in the techniques of both primary and repeat hepatopancreatobiliary interventions, have led to a significant reduction in postoperative purulent-inflammatory complications (to 2.63%, compared with 5–6% according to annual reports from the previous five years). Conclusion. The potentially serious outcomes of postoperative purulent-septic complications require further refinement of preventive measures and management strategies.
Introduction. Colorectal cancer (CRC) remains one of the most common causes of cancer incidence and mortality, particularly among older adults. Population aging and increased life expectancy contribute to a growing proportion of elderly patients diagnosed with CRC. Considering comorbidities, functional limitations, and a high risk of complications, the choice of optimal surgical management in this population is challenging. Therefore, comparative analyses of different surgical strategies in this patient group present clinical significance. The aim of this study was to perform a comparative analysis of surgical outcomes in elderly patients with colon cancer depending on a surgical approach. Materials and methods. The study included 140 patients who underwent either laparotomic or laparoscopic surgery. Demographic and clinical and pathologic features, intra- and postoperative parameters, complication rates according to the Clavien—Dindo classification, as well as survival outcomes, were assessed. Results. Laparoscopic interventions were associated with shorter hospital stays, while overall survival rates were comparable between the two groups. The frequency of postoperative complications according to the Clavien—Dindo classification was similar; however, grade II complications occurred more frequently in the laparotomy group. No statistically significant differences were observed in postoperative mortality or disease stage between the groups. Discussion. Both current literature and the obtained results confirm the safety and effectiveness of the laparoscopic approach in elderly patients with CRC. Minimally invasive interventions are associated with reduced intraoperative trauma and more favorable postoperative recovery. Nevertheless, careful preoperative selection remains essential, particularly in patients with severe comorbidities. Conclusion. The findings indicate that minimally invasive procedures are safe and highly effective in the surgical management of colorectal cancer in elderly patients.
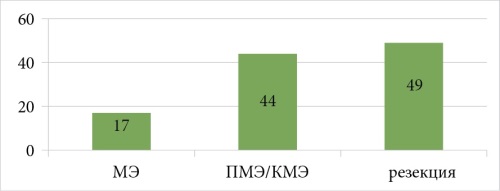
Introduction. This article presents the study of 110 female patients diagnosed with stage 0 breast cancer conducted at the P. Hertsen Moscow Oncology Research Institute between 2023 and 2024. Materials and methods. By histological type, ductal carcinoma in situ (Tis, DCIS) predominated in 100/110 cases (90.9%), followed by Paget’s disease (Tis, Paget) in 7/110 (6.4%), and lobular carcinoma in situ (Tis, LCIS) in 3/110 (2.7%). Mastectomy was performed in 17 patients (15.5%), skin-sparing mastectomy with reconstruction in 44 (40%), and breast-conserving surgery in 49 (44.5%). Results. According to routine histological examination, progression of DCIS was identified in 42/110 patients (38.2%). Among them, stage I breast cancer was diagnosed in 33.6% and stage II in 4.5%. In routine morphological examination, positive resection margins (R1) were detected in 15 patients (13.6%). Discussion. Breast MRI in non-invasive breast cancer is an essential procedure for determining disease extent, assessing multifocality or multicentricity, and thus guiding the decision on breast-conserving surgery versus mastectomy. Another important issue is the need to evaluate sentinel lymph nodes in cases of non-invasive breast cancer. Conclusion. Local recurrences of breast cancer in the analyzed group were diagnosed in 2 patients (1.8 ± 1.6%). Progression of stage 0 breast cancer to higher stages, i.e., cTis → pT+, was observed in 42/110 patients (38.2%). Despite the extent of disease (mean size of carcinoma in situ was 42 mm), breastconserving surgery or nipple-/skin-sparing mastectomy with reconstruction were performed in 93% of cases. Thus, carcinoma in situ may progress to higher stages in about 40% of patients. The role of diagnostic methods in assessing breast cancer stage is therefore crucial for selecting an optimal surgical management.
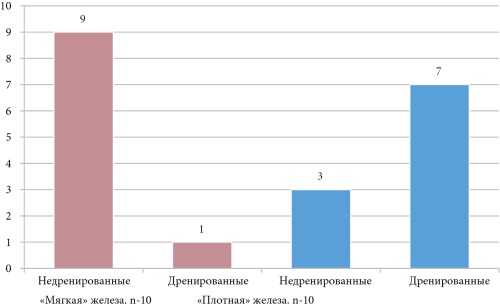
Introduction. Gastro-pancreaticoduodenal resection remains the only radical treatment of biliopancreatic and duodenal malignancies. However, this procedure is associated with a high likelihood of postoperative complications. Among them, delayed gastric emptying (DGE) is the most common, although its etiology is still unclear. While DGE is not a life-threatening condition, it significantly prolongs hospitalization, increases treatment costs, and delays the initiation of adjuvant chemotherapy. The aim of this study was to evaluate the effectiveness of treatment modalities and summarize the clinical experience of managing patients with DGE. Materials and methods. The study was conducted at the I.K. Akhunbaev Clinic of the National Hospital of the Ministry of Health of the Kyrgyz Republic, Bishkek. Between 2009 and 2023, 85 gastro-pancreaticoduodenal resections were performed for biliopancreatic and duodenal malignant neoplasms. The study group included 69 men and 16 women, with a mean age of 57.5 ± 1.4 years. Results. In patients with pancreatic adenocarcinoma, DGE developed in 24% of cases, while in those with neuroendocrine tumors, it was observed in 75% of cases. Among patients with “soft” pancreatic parenchyma, DGE occurred in 28.6%, whereas in those with “firm” parenchyma, the incidence was 19.2%. Correlation analysis between parenchymal characteristics and the development of DGE showed statistical significance (P ≤ 0.05). Discussion. In patients with tumors in the periampullary region, the overall incidence of DGE was 23.5%. The identified risk factors for DGE included pancreatic parenchymal consistency, presence of obstructive jaundice, tumor histotype, and patient age. Early recognition of these risk factors may enable preventive measures against DGE in the postoperative period. Prophylactic administration of erythromycin, as recommended by randomized trials, accelerates the resolution of DGE, which was confirmed by clinical outcomes. Conclusion. Gastro-pancreaticoduodenal resection is one of the most complex operations in abdominal surgery, both technically and postoperatively. It carries a high risk of complications. Identifying risk factors may help elucidate the mechanisms behind complications such as delayed gastric emptying and pancreatic fistulas.
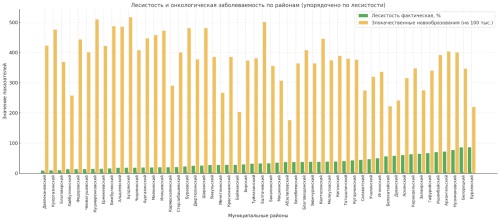
Introduction. The health status of the population is an important indicator of environmental quality and social well-being. In recent decades, the number of diseases associated with deteriorating air quality has grown. Malignant neoplasms occupy a special place among them. It has been established that carcinogenic chemicals present in air, water, and soil can cause DNA replication errors and impair immune surveillance, thereby increasing the risk of oncological diseases. The aim of this study was to examine the relationship between the degree of forest cover and cancer incidence in the municipal districts of the Republic of Bashkortostan, to assess the impact of environmental factors on public health, and to determine their role in cancer prevention. Materials and methods. This was a retrospective, correlational study. Data from 2024 were analyzed for 54 municipal districts of the Republic of Bashkortostan. The main data sources included official reports from oncology services, Rosstat, the Ministry of Ecology of the Republic of Bashkortostan, and geoportals. Methods of spatial ecology and multiple linear regression were applied, with calculation of regression coefficients, p‑values, confidence intervals, and the coefficient of determination. Results. A statistically significant inverse relationship was identified between the degree of forest cover and cancer incidence: a 1% increase in forest cover was associated with a decrease of 1.825 cases per 100,000 population (p = 0.001, R² = 0.200). When the variable “availability of oncologists” was added, the relationship remained significant (p = 0.002). Spatial analysis confirmed the identified patterns. Discussion. The findings support the hypothesis of a protective role forest ecosystems play against environmental carcinogenic factors. Protective mechanisms include absorption of air pollutants, deposition of particulate matter, and biodegradation of heavy metals. Despite the lack of statistically significant influence from medical staffing, the ecological factor proved to be independent. Conclusion. The established relationship between forest cover and reduced cancer incidence necessitates integration of ecological aspects into public health protection strategies. The data obtained may serve as a scientific basis for regional programs of ecological rehabilitation and preventive interventions.
Introduction. Papillary thyroid carcinomas (PTC) are considered relatively common occult and incidental findings, with generally good prognosis and favorable outcome. Despite this, metastases to the central lymph nodes (CLN) occur frequently and are associated with adverse consequences and prognosis for patients. The aim of the present study was to assess the frequency of central lymph node metastases in patients with papillary thyroid carcinoma staged as pT1a over a 10-year period, and to identify possible risk factors associated with the presence of CLN metastases. Materials and methods. A retrospective cohort study was conducted at the Interterritorial Endocrine Surgery Center, Krasnodar. Between January 2010 and January 2022, thyroidectomy was performed in 3013 patients. A total of 2818 patients were excluded from the study following thyroidectomy due to final benign histological findings, age under 18 years, follicular, medullary, anaplastic carcinoma, mixed-type thyroid carcinoma, tumor size > 1 cm, and stages pT1b–pT4. The analysis included 195 patients with pT1a papillary thyroid carcinoma. All patients underwent thyroidectomy and prophylactic or therapeutic standardized lymph node dissection. Results and discussion. Multivariate analysis demonstrated that central lymph node metastases were present in a significant number of cases in patients with PTC after organ preservation surgery. Therefore, in order to choose the most effective surgical treatment, careful preoperative evaluation is warranted for patients without confirmed lymph node metastases (N0). Conclusion. The results of our study indicate that CLN metastases are present in a considerable proportion of patients with PTC after thyroid resection. Combining these findings with preoperative ultrasonography may assist clinicians in accurately assessing whether CLN metastases are present in patients with PTC, thereby facilitating appropriate surgical planning for each individual patient.
Introduction. Ovarian cancer is the ninth most common malignant neoplasm. This condition often causes severe complications, such as loss of reproductive organs, which is particularly characteristic of hereditary forms of the cancer. At present, a wide range of ovarian cancer treatments is available, including targeted therapy; however, optimal immunotherapy regimens are still lacking. The development and progression of ovarian cancer are largely determined by impaired immune surveillance. A factor influencing the effectiveness of immune surveillance of the tumor is a diverse repertoire of T-cell and B-cell receptors. The aim of this study was to investigate the levels of T-cell receptor excision circles (TREC) and κ-deleting recombination excision circles (KREC) in patients with stage I–III ovarian cancer. Materials and methods. Levels of TREC and KREC were analyzed in 42 patients with ovarian cancer who underwent radical treatment. The study included patients aged 23 to 74 years. Results and discussion. The median TREC level (copies/10⁵ cells) was 16.04 [Q1–Q3: 2.14–37.31], and the median KREC level (copies/10⁵ cells) was 130.06 [Q1–Q3: 0.34–917.00]. Following radical treatment, 17 patients (40.5%) experienced disease recurrence. The median recurrence-free survival was 19 months, with the earliest recurrence observed 7 months after surgery. Our findings corroborate previous studies indicating an association between malignant tumor progression and excision circle levels. The results also demonstrated a decrease in TREC and KREC levels with increasing patient age, as well as a clear trend toward recurrence in patients with reduced blood levels of TREC and KREC. Conclusion. Based on our results, in patients with recurrent ovarian cancer, blood levels of TREC and KREC are low. These changes reflect the presence of immunodeficiency conditions, which in turn indicate reduced antitumor.
Introduction. Acute necrotizing pancreatitis (ANP), a severe acute pancreatitis accompanied by necrosis, is associated with high morbidity and mortality. Traditional management has shifted toward minimally invasive multimodal strategies, though a choice of optimal drainage procedures is still being debated and requires evidence-based guideliness. Aim: To analyze ANP outcomes and develop an effective minimally invasive drainage algorithm to reduce complications, mortality, and length of hospitalization. Materials and methods. A prospective study (2019–2024) included 136 ANP patients managed according to necrosis score versus 140 historical controls. Necrosis extent was defined using Revised Atlanta Cclassification: mild (≤30%), moderate (30–60%), extensive (>60%). Interventions included ultrasound-guided drainage, laparoscopic necrosectomy, and early open debridement. Conservative treatment comprised antibiotics, prolonged epidural analgesia, enteral feeding. Outcomes were assessed using SAPS, APACHE II/III, MODS, and SOFA scores. Statistical analysis compared frequency of complications, mortality and length of hospitalization. Results. Protocol cohort showed significant improvements: Mild necrosis: Infections ↓ to 11.1% (vs. 23.6%; *p* = 0.01), mortality ↓ to 1.1% (vs. 5.2%; *p* = 0.03). Modertae necrosis: Laparoscopic necrosectomy reduced sepsis to 37.7% (Δ = 41.1%; *p* < 0.001), mortality ↓ to 11.4% (vs. 28.3%; *p* = 0.002). Extensive necrosis: Early open debridement ↓ endotoxicosis mortality to 13.7% (vs. 41.2%; *p* = 0.007), overall mortality ↓ to 34.4% (vs. 62.1%; *p* = 0.01). Overall, protocol adherence ↓ infections by 65% (21.7% vs. 62.8%; *p* < 0.001), mortality by 24% (12.4% vs. 16.4%; *p* = 0.03), and lengths of hospital stays by 22% (58 vs. 74 days; *p* = 0.002). Discussion. This study validates a necrosis score protocol as superior to historical approaches. Minimally invasive techniques are definitive for mild/moderate necrosis, while early open debridement is critical for extensive necrosis. Key innovations (epidural analgesia, early enteral nutrition, step-up drainage) synergistically reduced systemic inflammation and sepsis. The 65% infection reduction underscores protocol efficacy, though multicenter validation is warranted. Conclusion. A tailored approach significantly improves ANP outcomes, offering a resource-efficient template for management.
REVIEWS
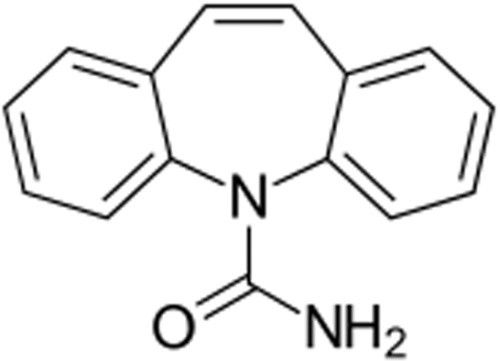
Glioblastoma is a malignant brain tumor characterized by an aggressive course, resistance to chemoradiation and immunotherapy, recurrence, and high mortality. The incidence of glioblastoma ranges from 3.2 to 5 per 100,000 people. In recent years, an increase in the incidence of glioblastoma among patients under 45 years of age has been observed. Epilepsy develops in 25–60% of the patients, reducing their quality of life and worsening the prognosis of the disease. In 35–40% of the patients, epileptic seizures are the first manifestation of glioblastoma, being also possible during its treatment or relapse. The risk of epilepsy development and its severity are affected by the tumor volume, growth pattern, localization, presence of preoperative seizures, IDH1-2 mutations, and residual tumor volume. The epilepsy associated with glioblastoma is characterized by a multifactorial and poorly understood etiopathogenesis. The leading role in epileptogenesis is attributed to dysfunction of ion channels with an increase in the level of extracellular K+, hyperexpression of SCN1A and SCN2A alpha subunits of Na+ channels, as well as dysregulatory Ca2+ channels. As a result, in the peritumoral zone, the homeostasis of inhibitory and excitatory neurotransmitters, repolarization/depolarization processes, and electrochemical interactions between neurons and tumor cells are disrupted. Due to its high clinical effectiveness, carbamazepine is most often used to treat glioblastoma-associated epilepsy. The antiepileptic activity of carbamazepine is related to the inactivation of Na+ channels, potentiation of potential-dependent K+, Cl–channels, the GABA-ergic system, inhibition of glutamate release, and the effect on the homeostasis of other neurotransmitter systems in the brain. The ability of carbamazepine to suppress cell proliferation in a number of malignant glioma cell lines is also of high significance. Although carbamazepine is an inducer of liver microsomal enzymes, it does not reduce the effectiveness of temozolomide, which is not metabolized in the liver. Possible adverse carbamazepine-associated reactions do not require its discontinuation. Given the high clinical effectiveness of carbamazepine, further studies of its pleiotropic effects in patients with epilepsy associated with glioblastoma and other malignant brain tumors are required.
CLINICAL CASES
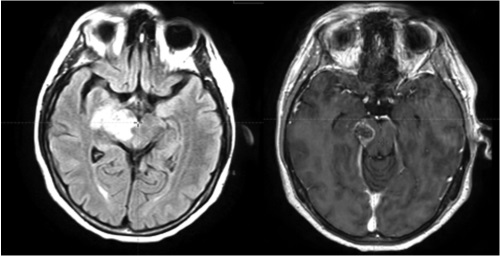
Introduction. Brainstem gliomas are associated with the median overall survival of 6–16 months. The available treatment approaches have not shown significant improvement in survival rate, which makes the search for improved strategies particularly relevant. Materials and methods. In Radiotherapy Unit No. 1 of the Voronezh Regional Scientific and Clinical Oncology Center, a patient with a clinical and radiological diagnosis of glioma grade 4 of the right thalamus, posterior limb of the internal capsule, and right cerebral peduncle was treated. Treatment strategy: conventional radiotherapy to 60 Gy with temozolomide 75 mg/m2 /day. Results. The prescribed dose for the affected area outside the brainstem was 60 Gy, including the brainstem — 56 Gy. The treatment was tolerated well. No toxicity or neurological deficit progression was observed. Discussion. According to most scientific publications, radiation therapy with 54 Gy is a confirmed therapeutic option in the treatment of brainstem gliomas. Some studies showed the possibility of increasing the maximum tolerant dose to the brainstem to 64 or 69.59 Gy. Therefore, the selected prescribed dose in the considered clinical case appears underestimated. However, during the planning process, the task was set to achieve a uniform dose distribution. In the future, in cases of primary brainstem formations, it seems advisable to use 58 Gy as the prescribed dose. Conclusion. In the clinical case under consideration, the delivery of the prescribed 56–60 Gy dose to the main volume of brainstem glioma is possible, taking into account the existing tolerance criteria with the achievement of satisfactory dose coverage and the absence of development of serious neurological complications.

ISSN 2307-0501 (Online)





























