


ORIGINAL ARTICLES
Introduction. Pancreatoduodenectomy is among the most technically demanding procedures in abdominal surgery. Recent developments in minimally invasive techniques, particularly laparoscopic and robotic systems, have reshaped operative strategies. Robotic systems offer several technical advantages over conventional laparoscopy, which may be especially advantageous in pancreatic surgery. Aim. This study evaluated the effectiveness and safety of robot‑assisted pancreatoduodenectomy.
Materials and methods. This study was conducted in the surgical department of the BSMU Clinic from September 2020 to September 2025. 27 patients undergoing operative treatment were included. Group 1 comprised 12 patients who underwent robot‑assisted pancreatoduodenectomy; Group 2 included 15 patients who underwent an open procedure. Perioperative outcomes and early and late postoperative complications were assessed and stratified according to the Clavien–Dindo classification. Statistical analysis was performed using Microsoft Office 2024 and IBM SPSS Statistics 27, with statistical significance set at p < 0.05.
Results and discussion. Preoperative characteristics exhibited no significant difference between groups (p > 0.05). Intraoperatively, Group 1 had significantly lower blood loss (p < 0.001), although operative time was longer than in Group 2 (p < 0.001). Postoperatively, Group 1 demonstrated faster recovery of bowel function (p < 0.001) and a shorter hospital stay (p = 0.004). Although thirty‑day postoperative complications occurred more frequently in Group 2 (46.7%), the difference between groups was statistically insignificant (p = 0.419). The advantages of the robotic approach are attributed to reduced operative trauma and greater precision during dissection and reconstruction.
Conclusion. Robot‑assisted pancreatoduodenectomy is an effective and safe option for the radical treatment of tumors of the pancreaticoduodenal region.
Introduction. Advances in surgical management of breast cancer have substantially improved postoperative quality of life. Aim. This study compares short-term and long-term outcomes associated with a newly developed breast-conserving surgical technique in routine clinical practice.
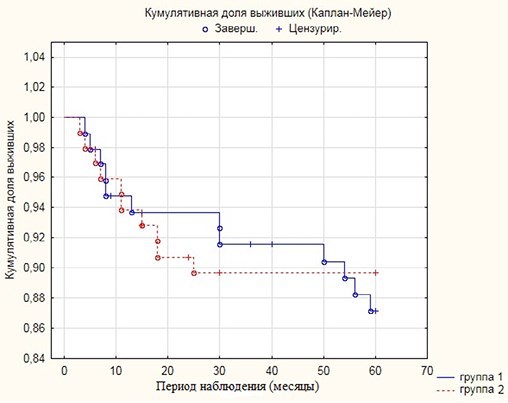
Materials and methods. A retrospective review was conducted of medical records from 194 women with histologically confirmed breast cancer treated at the Samara Regional Oncology Center (Samara, Russia) between 2011 and 2020. Based on the extent and characteristics of surgical intervention, patients were stratified into two groups: a control group (n = 96) that underwent standard breast-conserving surgery and a main group (n = 98) that was treated using a newly developed method for determining surgical volume. The technique involved securing the free edge of the lateral thoracoaxillary dermal-fat flap in the axillary region along the anatomical course of the long thoracic nerve. Operative time and intraoperative blood loss were recorded. Disease-free and overall survival were analyzed using the Kaplan–Meier method. Quality of life was assessed using the Breast-Q questionnaire preoperatively and 6 months after treatment. Parametric and non-parametric statistical methods were applied, with significance set at p < 0.05.
Results and discussion. Mean operative time was 76.3 ± 23.3 minutes in the control group and 65.5 ± 18.3 minutes in the main group (p < 0.001). Blood loss averaged 53.1 ± 26.2 mL and 49.0 ± 14.3 mL, respectively (p = 0.18). Persistent non-infected seroma occurred in 19 patients in the control group and 7 patients in the main group (p = 0.009). The developed technique was associated with a statistically significant reduction in postoperative complications, while long-term oncologic outcomes did not differ between groups.
Conclusion. Use of the newly developed breast-conserving technique significantly reduces postoperative complication rates without compromising long-term treatment outcomes.
Introduction. Ovarian cancer remains one of the leading causes of cancer‑related mortality among women. Globally, approximately 200,000 new cases and 100,000 deaths are reported annually. Most ovarian tumors are diagnosed at an advanced stage, while only 25–30 % are detected early. In advanced disease, the primary objective of surgical treatment is complete cytoreduction of all macroscopically visible disease, as this factor is strongly associated with improved overall survival and longer progression‑free intervals. Aim. This study evaluated the effect of complete cytoreductive surgery on early postoperative complications, mortality, and long‑term overall survival in patients with advanced ovarian cancer.
Materials and methods. We conducted a retrospective review of medical records for patients who underwent primary cytoreductive surgery for advanced ovarian cancer at the Kurgan Regional Oncology Center between 1 January 2017 and 1 January 2025.
Results and discussion. A total of 54 women underwent cytoreductive surgery. Complete cytoreduction was achieved in 90.7% (n = 49), while 9.3 % (n = 5) had residual disease. The number of adjacent organs resected ranged from 1 (53.6 %) to 5 (5.6 %), with a mean of 2.02 ± 1.28. Postoperative complications occurred in 51.9% (n = 28) of patients; grade IV complications occurred in 5.6 % (n = 3) and grade V in 1.9% (n = 1) according to the Clavien–Dindo classification. Mean operative time was 365.61 ± 176.08 minutes (range of 90–820 minutes). Importantly, patients who underwent complete cytoreduction did not exhibit higher rates of severe postoperative complications or mortality (Clavien–Dindo grades IV–V).
Conclusion. A more extensive surgical approach is justified in selected patients with advanced ovarian cancer and is associated with improved survival. However, careful patient selection is essential, as overall preoperative status may significantly influence survival outcomes.
Introduction. Prevention of bronchopleural fistula after bronchoplastic procedures for malignant lung tumors remains a major challenge in thoracic oncology. As a result, the search for reliable techniques to reinforce and cover bronchial sutures continues to be clinically important.
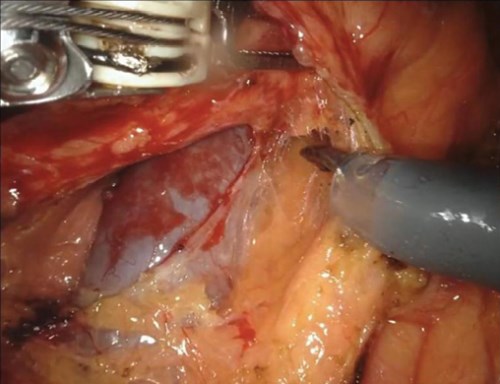
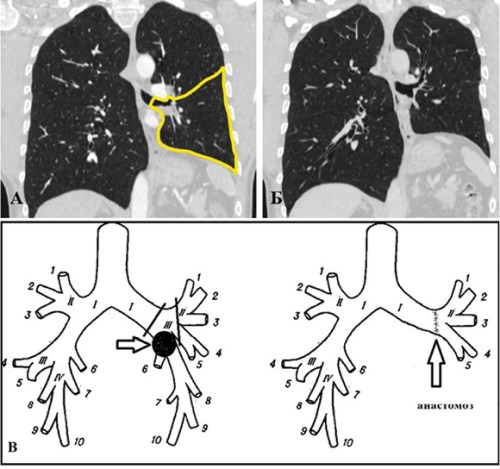
Materials and methods. Between 2021 and 2024, 17 elective bronchoplastic procedures were performed in the onco-thoracic department of the Chelyabinsk Regional Center for Oncology and Nuclear Medicine in patients with central non-small-cell lung cancer. The cohort included 7 circular bronchoplasties, 1 circular broncho-angioplasty, 1 circular bronchoplasty with a polybronchial anastomosis, and 8 wedge bronchoplasties. Three methods of additional bronchial suture coverage were used: a vascularized intercostal muscle flap (5 patients), a pedicled pleural‑fat flap (5 patients), and a free pleural‑fat flap harvested from the pericardial region (7 patients).
Results and discussion. No bronchopleural fistulas occurred in the postoperative period. Five patients experienced exacerbation of chronic bronchitis. One patient developed prolonged air leak with subcutaneous emphysema, and one patient had intrapleural bleeding. Postoperative empyema occurred in one patient and resolved after drainage and pleural lavage. At the time of publication, 15 patients were in remission. Two patients who underwent circular bronchoplasty died 7 and 8 months postoperatively due to tumor progression.
Conclusions. Routine coverage of bronchial sutures after bronchoplastic lung resections for malignant tumors is recommended to reduce the risk of bronchopleural fistula. The choice of flap should be determined by the operating surgeon.
Introduction. Although uncommon, biliary ileus is a severe complication of gallstone disease, occurring primarily in elderly patients and associated with high mortality. Aim. This study examined the clinical presentation, diagnostic features, and surgical management of biliary ileus and evaluated the effectiveness of different treatment strategies based on 15 years of clinical experience.
Materials and methods. A retrospective analysis was performed on 37 patients (32 women, 5 men; mean age 71.4 ± 9.6 years) treated in the surgical departments of three clinics in the Central region of Russia between 2010 and 2024. A cholecystoduodenal fistula was identified in 75.6% of cases, and the ileum was the most common site of gallstone impaction (62.1%).
Results. A strong association was observed between the stage of intestinal obstruction, the severity of hemodynamic disturbances, and the degree of endogenous intoxication. Mortality ranged from 7.5–10% in compensated obstruction, 15–20% in subcompensation, and 30–35% in decompensation. The primary surgical approach was isolated enterolithotomy (81.1%), which demonstrated the lowest complication rates (6.6%) and mortality (6.6%). In contrast, mortality after bowel resection reached 50%. Discussion. Radical procedures involving cholecystectomy and fistula repair are indicated only in patients with stable hemodynamics and acceptable somatic status. The degree of endogenous intoxication correlates with the severity of intestinal obstruction. These findings confirm that early diagnosis, careful hemodynamic assessment, and evaluation of endogenous intoxication are critical for selecting an appropriate treatment strategy.
Conclusion. An individualized approach and prioritization of organ‑preserving procedures reduce complication rates, shorten hospitalization, and improve prognosis in patients with biliary ileus.
Introduction. Laparoscopic surgery has become the standard of care for many abdominal conditions due to its minimal invasiveness, reduced postoperative pain, and shorter recovery times compared with open procedures. Continued technological development and refinement of operative techniques remain essential for improving clinical outcomes. This study analyzed five-year trends in the use of laparoscopic surgery and assessed its impact on the frequency and severity of postoperative intra-abdominal complications at the I.V. Davydovsky City Clinical Hospital (Moscow, Russia).
Materials and methods. A retrospective analysis was performed on 4,794 medical records of patients who underwent abdominal or retroperitoneal surgery between 2019 and 2023. The number and type of procedures, postoperative complication rates (Clavien–Dindo classification), and hospital length of stay were evaluated. Statistical methods were used to identify significant trends and correlations.
Results. The total number of operations increased from 574 in 2019 to 1,513 in 2023. The proportion of laparoscopic procedures rose from 31.18% to 63.45%. During the same period, the overall postoperative complication rate decreased from 11.15% to 1%. Analysis according to the Clavien–Dindo classification demonstrated reductions in both the frequency and severity of complications; no grade IV or V complications occurred in the laparoscopic group. A trend toward a shorter average hospital stay was also observed.
Discussion. The strong inverse correlation between the increasing proportion of laparoscopic procedures and the declining complication rate highlights the safety and effectiveness of minimally invasive surgery. Improved outcomes reflect both the intrinsic advantages of the laparoscopic approach and the accumulating experience of the surgical team (learning curve effect).
Conclusion. The systematic expansion of laparoscopic surgery within a specialized department markedly improves patient outcomes by significantly reducing the frequency and severity of postoperative complications. These findings support continued investment in surgical training, technological development, and the broader implementation of minimally invasive techniques to enhance patient safety and healthcare efficiency.
Introduction. Medullary thyroid carcinoma (MTC) is a rare and aggressive malignancy, accounting for 2–5% of all thyroid cancers. Aim. This study examined the epidemiological profile of MTC in the Tyumen Region (Russia) and evaluated the effectiveness and tolerability of multikinase inhibitors (MKIs) in MTC therapy.
Materials and methods. The analysis included 69 patients with MTC treated between 2017 and 2025. Patient age ranged from 39 to 78 years (median 57). Sonographic characteristics of thyroid nodules were classified according to the EU-TIRADS. Cytological evaluation of fine-needle aspiration samples followed the Bethesda Thyroid Classification (2009, 2017, 2023). Survival outcomes were calculated using the Kaplan–Meier method. Serum calcitonin (CT) and carcinoembryonic antigen (CEA) levels were measured by electrochemiluminescence. RET mutation testing was performed on blood samples and, in one case, on surgical tissue.
Results. Between 2017 and 2025, peak MTC incidence in the Tyumen Region occurred in 2021 and 2024, reaching 0.65 and 0.74 per 100,000 population, respectively. During cabozantinib therapy, mean survival was 19.30 months (95% CI 14.45–21.39), with a median of 17.01 months. For vandetanib in first-line therapy, mean survival was 18 months (95% CI 12.57–23.59), with a median of 14.00 months (95% CI 12.46–20.55). The objective response rate was 29.4% with vandetanib and 36.8% with cabozantinib. The most frequent adverse events were arterial hypertension with vandetanib, palmar-plantar erythrodysesthesia with cabozantinib, and toxic hepatitis with selpercatinib. Discussion. This retrospective analysis demonstrates the effectiveness and safety of MKIs in routine clinical practice. Cabozantinib showed superior survival outcomes and objective response rates compared to vandetanib. The observed adverse events were expected and manageable. The findings are consistent with published clinical evidence.
Conclusion. Given the aggressive nature of MTC, continuous monitoring of disease progression is essential. In cases of progression, MKI therapy should be considered, with careful evaluation of potential toxicity in relation to individual treatment goals.
Introduction. Breast cancer remains the leading cause of cancer morbidity and mortality among women. In hormone-receptor-positive, HER2-negative disease, achieving a pathologic complete response (pCR) after neoadjuvant therapy is an important prognostic factor. Aim. This study evaluates the efficacy and safety of adding tamoxifen to standard neoadjuvant chemotherapy in patients with hormone-sensitive, HER2-negative breast cancer.
Materials and methods. A prospective randomized study included 40 preand postmenopausal patients with indications for neoadjuvant chemotherapy using the 4ddAC → 4T regimen. Patients were assigned to two groups: Group A (n = 20) received additional tamoxifen, while Group B (n = 20) received chemotherapy alone. The primary endpoint was the pCR rate, assessed using the Residual Cancer Burden (RCB) system.
Results and discussion. The pCR rate (RCB-0) was 10% in both groups. The distribution of residual tumor burden across RCB classes was similar, with no statistically significant differences (p > 0.05). Combined chemo-hormonal therapy demonstrated acceptable tolerability; no serious adverse events were reported. All patients completed treatment and subsequently underwent surgery. The addition of tamoxifen did not improve the likelihood of achieving pCR, confirming its limited role in this neoadjuvant regimen.
Conclusion. The study demonstrated comparable efficacy and safety between the two treatment strategies. The absence of benefit from adding tamoxifen highlights the need to explore new therapeutic approaches to improve outcomes in this patient population.
CLINICAL CASES

Introduction. Combat-related injuries to major limb vessels pose a threat to both life and limb. Although clinical management traditionally prioritizes restoration of arterial inflow, the contribution of venous injury to limb ischemia is often underestimated.
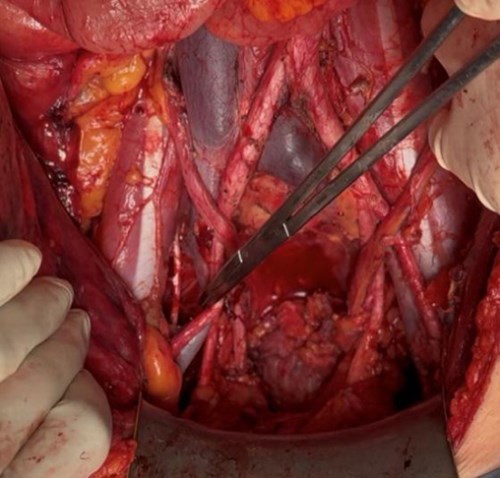
Material and methods. We describe the case of a 22-yearold serviceman with multiple blind shrapnel wounds of the right thigh that resulted in grade III acute ischemia of the right lower extremity.
Results and discussion. Intraoperative examination identified a popliteal vein rupture with a 4-cm gap between the stumps, while the popliteal artery remained intact. Autologous venous reconstruction of the popliteal vein was performed using a resected small saphenous vein graft (with a length of 4 cm and a diameter of 1 cm). Within 30 s of restoring venous outflow, pulsation of the popliteal artery and antegrade flow in the tibial arteries were recorded. The procedure was supplemented with a fasciotomy of the lower leg. The postoperative course was uneventful. This case demonstrates that severe impairment of venous drainage, leading to venous hypertension and stasis, may clinically mimic arterial occlusion and present as critical ischemia. Restoration of venous outflow resolved the ischemia without the need for arterial reconstruction.
Conclusion. Isolated popliteal vein injury can lead to critical limb ischemia due to venous congestion.

Introduction. Primary sclerosing cholangitis (PSC) is a chronic progressive disease of the liver and biliary tract characterized by inflammation and fibrosis of the bile ducts, leading to multifocal strictures, impaired bile flow, cholestasis, and ultimately hepatolithiasis. One therapeutic option for this complication is endoscopic retrograde cholangiopancreatography (ERCP) with direct visualization using the SpyGlass DS system.
Materials and methods. This article describes a clinical case of a PSC progressing to liver cirrhosis and complicated by hepatolithiasis and choledocholithiasis. The clinical course was further aggravated by concomitant ulcerative colitis.
Results and discussion. A staged approach, including endoscopic retrograde papillotomy, cholangiopancreatography, and direct cholangioscopy using SpyGlass DS, enabled the complete removal of biliary stones and restoration of normal bile drainage.
Conclusion. The combined use of endoscopic retrograde papillotomy, cholangiopancreatography, and direct cholangioscopy with the SpyGlass DS system provides effective diagnostic and therapeutic management of hepatolithiasis. An individualized, multidisciplinary approach contributes to improved clinical outcomes.

Introduction. Intestinal fistulas remain among the most challenging and discouraging complications in abdominal surgery. Their diverse morphology, profound pathophysiological disturbances of homeostasis, and the complexity of management strategies, ranging from conservative management to surgical intervention, contribute to high mortality and suboptimal treatment outcomes. Aim. This report describes successful conservative treatment of an unformed small-bowel fistula using negative-pressure wound therapy (NPWT).
Materials and methods. We report the case of a 70-year-old woman who developed an unformed small-bowel fistula following closure of a loop protective ileostomy. NPWT was applied to the abdominal wall wound using continuous suction at –70 mmHg. Treatment began with a porous polyurethane sponge and concluded with suction applied without a sponge. This approach resulted in progressive reduction of the wound cavity, a significant decrease in fistula output, and eventual spontaneous closure. The postoperative course, local wound-care technique, medications used, treatment stages, and duration of therapy are described. The patient achieved full recovery with rapid fistula closure.
Results and discussion. A review of the recent literature is provided, including reports on the use of NPWT for gastrointestinal fistulas. Evidence indicates that NPWT may facilitate spontaneous closure of gastrointestinal fistulas or promote formation of a low-output, well-defined fistula suitable for elective surgical repair. These outcomes are attributed to drainage of purulent cavities, reduction of fistula output, protection of the abdominal wall skin, and progressive reduction of wound size. These are recognized effects of negative pressure on soft tissues.
Conclusion. Negative-pressure therapy is an appropriate option for unformed small intestinal fistulas and frequently enables successful conservative management.
Introduction. Total pancreatoduodenectomy is among the most technically demanding procedures in abdominal surgery, both in terms of operative complexity and perioperative management. It is performed as a necessary alternative to standard pancreatoduodenal resection in cases of intraductal pancreatic cancer with diffuse gland involvement. Aim. This study describes the technical features and perioperative management of patients undergoing total pancreatoduodenectomy.
Material and methods. From 2019 to the present, 99 operations for pancreatic cancer were performed in the First Surgical Department of the Republican Clinical Hospital named after G.G. Kuvatov. These included 14 distal (corporal-caudal) pancreatectomies, 78 pancreatoduodenal resections, and 7 total pancreatoduodenectomies. All seven total pancreatoduodenectomies were performed for pancreatic ductal adenocarcinoma complicated by obstructive jaundice. The initial stage involved percutaneous transhepatic external biliary drainage. Intraoperatively, hemodynamic stability was maintained through transfusion of packed red blood cells, plasma, and crystalloids. Blood glucose was monitored every 60 minutes and maintained between 6.0 and 10.0 mmol/L using short-acting insulin.
Results and discussion. The duration of total pancreatoduodenectomy was significantly longer than that of standard pancreatoduodenal resection (p < 0.05), despite fewer anastomoses. Estimated blood loss was comparable between procedures. One 73-yearold patient died in the early postoperative period due to an acute myocardial infarction. Four patients died during long-term follow-up; two remain under observation at 14 and 4 months without evidence of disease progression. Median survival was 14.2 months. Total pancreatoduodenectomy, performed as a necessary measure in ductal pancreatic cancer with subtotal or total gland involvement, remains a highly traumatic procedure. Nevertheless, advances in surgical technique, anesthesiology, and critical care support justify its use in specialized centers.
Conclusion. Total pancreatoduodenectomy is an extensive and high-risk procedure that can be performed safely in specialized institutions with appropriate surgical and perioperative expertise.

ISSN 2307-0501 (Online)





























