


ORIGINAL ARTICLES
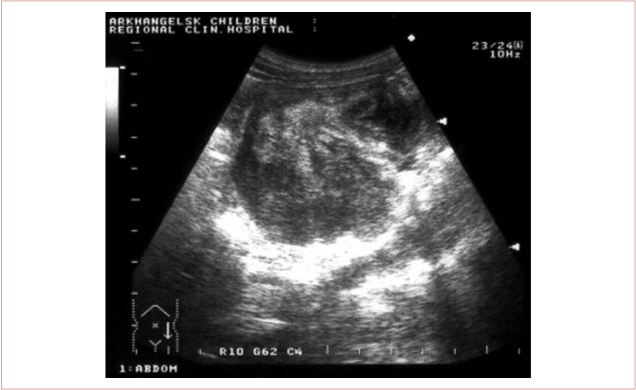
Introduction. A nonsurgical reduction is the treatment of choice for intestinal intussusception. A neoplasm-associated intussusception always requires surgery. In case of a tumour it is very important to have the diagnosis determined prior to surgical treatment. The hydrocolonic sonography technique makes it possible to assess the tissue structure and to visualize the lumen of the intestine.
Materials and methods. The study presents a retrospective comparative analysis of clinical manifestations and diagnosis methods in all the patients with intussusception (n = 380) treated at the Arkhangelsk Children’sClinicalHospital in 1981–2018. This included all the neoplasm-associated intussusception cases (tumours and polyps). The data was compared to clinical manifestations of intussusception associated with other causes (idiopathic, mesenteric node hyperplasia, diverticulum).
Results. Neoplasm-associated intussusception is a rare occurrence (2.3%). If the cause of the intussusception is a tumour the typical recorded manifestations include the combination of the signs of gastrointestinal diseases and loss of weight (8–12%), and a chronic course of development (over one to three months). Polyp-associated small intestinal and ileocolic intussusception, a casuistically rare situation, first manifested as an acute intestinal obstruction with protracted abdominal pain syndrome in anamnesis, or recurrent intussusceptions. Traditional and hydrocolonic sonography made it possible to make the diagnosis of intussusception and to identify a tumour. Non-tumour-associated intussusception presented with an acute course of the disease in every case. It manifested with the typical triad of symptoms (abdominal colic pain, rectal haemorrhage, palpable intussusceptum mass) in every third case. The manifestation of the disease as the dyad of symptoms (vomiting and abdominal colic pain) was significantly more frequent (p = 0.001).
Conclusions. Clinical presentation of neoplasm-associated intussusception has certain unique qualities. The ultrasound of abdominal cavity and hydrocolonic sonography make it possible to find the intussusception and to identify the tumour or polyp in the structure of the intussusceptum in 100 % of cases at primary examination. The data obtained is used for the optimisation of the surgical treatment strategy.

Introduction. Acute appendicitis takes the first place in incidence among acute surgical disorders of the abdominal cavity organs. While many issues of the diagnosis and treatment strategy of this disease have been studied in detail, the diagnosis of acute appendicitis remains primarily a matter of clinical presentation. National guidelines on acute appendicitis also recommend additional methods for a number of stipulated situations; these methods include the Alvarado score. The key goal of this study is to analyse the results of using the Alvarado score in the diagnosis of acute appendicitis and juxtaposing these results with the laparoscopic and pathomorphological data.
Materials and methods. This non-randomised prospective study presents the analysis of examination and treatment of 4,941 patients with acute appendicitis from the two periods — from 2006 to 2010 and from 2011 to 2015 — which is before and after the Alvarado score was introduced into the examination protocol. The likelihood of acute appendicitis according to the Alvarado score is evaluated as follows. A score of one to four is interpreted as appendicitis is unlikely; a score of five or six — acute appendicitis is possible, further dynamic observation is required; a score of seven to ten indicates a most probable acute appendicitis.
Results and discussion. The total sensitivity of the scoring system exceeded 90%; however, it did not result in a reduction of the number of diagnostic laparoscopies.
Conclusion. The authors see as the upsides of the use of the Alvarado score the improvement of the diagnostic precision and the reduced incidence of catarrhal appendicitis (down to 0.1%) and gangrenous forms of appendicitis (from 14.6% to 8.9%) due to a shorter observation period. The authors explain the failure to achieve the result planned by the healthcare funding costs and the drive to obtain a more precise diagnosis.

Introduction. The incidence of pancreatic pseudocysts (PPC) amounts to 0.5–1 per 100,000 adults per year. In all the pancreatic disorders the incidence of PPC amounts to 1.6-4.5%. Designing an individually tailored treatment programme using minimally invasive techniques to ensure the longest lasting treatment effect combined with the reduction of surgical trauma is an important issue of today’s surgery.
Materials and methods. This paper presents a retrospective analysis of surgeries performed on 101 patients with infected PPC treated in the period from 2000 to 2015 at surgical wards of the Centre for Emergency and Disaster Medicine of the Regional Teaching Hospital, Kharkiv, Ukraine and the Department of Pancreatic and Bile Duct Surgery of A. A. Shalimov National Institute of Surgery and Transplantology, Kyiv, Ukraine. Of these, 74 patients (73.3%) were male and 27 (26.7%) — female, aged 21 to 79, average age of patients was 43.3±1.2 years.
Results. Percutaneous drainage was administered to patients with type I infected PPC with the onset of multiple organ failure in order to make the wait-and-see strategy possible and to alleviate the patient’s general condition and improve the course of sepsis. For patients with type II and III infected PPC percutaneous punctures were the final stage of treatment in 80% of cases. Whether radical surgical procedures were performed depended on the severity of the patient’s condition, degree of pancreatic necrosis or chronic pancreatitis spread, PC localisation, duct system condition and complications involving neighbouring organs.
Conclusion. When treating patients with PPC one has to use an individually tailored treatment strategy based on state of the art minimally invasive treatment techniques. When treating infected PPC both minimally invasive and traditional open access procedures have to be considered as mutually complementing, presenting a broad range of diagnostic and treatment options.

Introduction. Graves’ disease is a disorder associated with thyroid gland producing excessive amounts of hormones which causes changes in the functional status of various organs and systems. Among thyroid disorders it takes the second place (after endemic goitre) in prevalence. Until now, there is no consensus on a single strategy for the treatment of disorders of the thyroid gland. This is why this paper aims to assess the impact of surgical treatment of Graves’ disease on patients’ quality of life and whether it would be possible to improve it by following the surgery with hormone replacement therapy.
Materials and methods. This paper presents a retrospective analysis of 70 case histories of patients who received surgical treatment for diffuse toxic goitre at the BIH UR “First Republican Teaching Hospital” MH UR,Izhevsk, in the period from 2008 to 2014. Percentages of the disease by stage were as follows: stage II — 20%, stage III — 70%, stage 4 — 10%. One lobe resection was performed in 3% of patients, two lobe resection — in 1%, hemithyroidectomy — in 18±4.6%, subtotal resection — in 8%, thyroidectomy — in 70±5.5%.
Results. Percentages of patients with various degrees of severity of postoperative hypothyroidism were as follows: severe — 66%, medium — 29%, light — 5%; there were no Graves’ disease recurrences. Patients’ complaints following thyroidectomy included body weight gain — 79.1±4.8%, cold in extremities — 83.3±4.4%, cardiac arrhythmia — 85.2±4.2%, oedemas — 84.3±4.3%, drowsiness, atonia — 67.1±5.6%, changes in appetite — 21±4.8%, skin pallor — 47.6±5.9%, brittle nails, hair loss — 51.2±5.9%, joint pain — 31.2±5.53%.
Conclusion. Hypothyroidism always follows thyroidectomy and requires ongoing hormone replacement therapy with L-thyroxine. Th quality of life does not have to suffer if an individual dosage is established and followed on a permanent basis.

Introduction. The ingrown nail (onychocryptosis) is a disease that is common both among children and in adult population. Despite the fact that there is a large number of methods available for the treatment of ingrown nails, a large percentage of recurrence of the disease remains unconquered. Traditional methods of treatment today are often complemented by chemical matrixectomy, cryodestruction, electrocoagulation or laser destruction of the growth zone of the nail plate piece being removed. The purpose of all of these methods of treatment is the reduction of the recurrence of the disease. This study aims to examine the possibilities of using a portable diode laser scalpel for the treatment of ingrown nails in children.
Materials and methods. In this study the authors compared treatment outcomes in patients with ingrown toenails treated with the original Winograd procedure (30 patients) with those treated with the same procedure complemented by the laser destruction of the growth zone (50 patients).
Results and discussion.There was one relapse case in the study group (n=50, 2%), and two — in the control group (n=30, 6.7 %). The healing period of the postoperative wound amounted to 17.3±2.05 days in the study group and to 12.25±1.24 days in control. Pain VAS scores on the first day following the surgery were 6.2±1.24 in the study group, and 5.8±0.816 in control. Staphylococcus aureus was the pathogen responsible for the local infection process in most patients with ingrown nails.
Conclusion. This study demonstrates that using the method proposed results in the reduction of the risk of recurrence of the disease from 6.7% down to 2%, increasing, however, the healing time of the postoperative wound from 12.25±1.24 to 17.3±2.05 days. This makes the use of the method proposed advisable in patients with:
a stage III ingrown nail;
an apparent local infectious process;
a recurrent ingrown nail.
Introduction. Currently the surgical treatment of inguinal hernias in children is usually a high ligation of the hernia sac without the separation of its distal portion or plastic reconstruction of the inguinal canal. This technique is considered the treatment of choice as it has brought down the incidence of post-operative hernias and testicular atrophy. However, the issues of approach to the selection of a conservative treatment strategy and the role played by instrumental examination methods used to determine indications for surgical treatment remain controversial.
Materials and methods. This paper presents a retrospective analysis of 684 clinical cases followed up at the Yaroslavl Regional Children’s Teaching Hospital. The study included boys aged one month to 17 years who were treated for inguinal and inguinoscrotal hernias in 2011-2015.
Results and discussion. 89 patients (10.3%) were hospitalised with incarcerated inguinal and inguinoscrotal hernias in the period under review. Of these, in 86 patients, when the incarceration lasted under 12 hours, conservative treatment attempts were undertaken. Hernia reduction was achieved without any direct manipulation on the hernia sac in 10 boys (11.6%). Attempts of manual hernia reduction were undertaken in the remaining 56 children (65.1%); these resulted in successful outcomes in 47 patients (83.9%). Emergency surgical repair of incarcerated hernias was performed in 23 cases (3.1%). No patients with incarcerated hernias were older than seven years. 45 out of 183 boys (29.5%) had scrotal oedemas and haematomas in the early post-operative period following planned hernia repair surgeries.
Conclusion. In the majority of patients hospitalised early the conservative hernia reduction approach was effective and resulted in fewer emergency hernia repair surgeries. Ultrasound examination of inguinal canal may be considered as a method of screening for asymptomatic hernias.

Introduction. Traumatic amputations of a thumb may happen as a result of severe mechanical injuries with the primary detachment and destruction of tissues, or following deep burns, frostbites or ischemia. In 70 to 80% of cases of disability and the loss of occupational fitness the key causes are traumatic digit and hand amputations. In 50% of cases the loss of ability to work is due to an amputation of a thumb. This makes the issue of thumb reconstruction a priority in surgery of the hand.
Materials and methods. This paper presents our experience in the reconstruction of the functional abilities of the hand in 48 patients with traumatic amputations of a thumb. This was performed with the use of reconstructive plastic microsurgery techniques, namely the free transplantation of a second toe onto the hand. All the patients had a thumb stump at the level of the distal part of the metacarpal bone or the proximal part of the proximal phalanx.
Results and discussion. A positive outcome was achieved in 45 out of the 48 patients treated. Autograft necrosis occurred in three cases. For these patients the thumb reconstruction was performed with the use of other, less functional methods. The functional condition of the hand manifested an improvement according to the electromyography data obtained at the maximum tonic tension of the thenar eminence muscles, flexor and extensor muscles of the reconstructed digit. In all the cases the hand strength increased by 40 to 90% after the reconstructive surgery; the authors attribute this to the recovery of the key handgrip abilities. According to Doppler ultrasonography data the blood flow velocity and the level of blood filling increased in the hand treated.
Conclusion. The reconstruction of functional abilities of the hand with traumatic thumb amputation must be carried out taking into account the available methods of surgical correction and which one of these would be optimal, the evaluation of the patient’s mental status and his or her drive for the fastest possible recovery of the shape and function of the hand. The free autograft of a second toe in place of the lost thumb with microsurgical vascular anastomoses makes it possible to restore most completely the aesthetic and functional abilities of the hand in the shortest possible timeframe.
REVIEWS
Introduction. Despite the fact that clinical studies of pulmonary surfactants conducted over many years have demonstrated their efficacy for the treatment of acute respiratory distress syndrome (ARDS) which led to their approval for use inRussia andBelarus, only a few similar positive results have been achieved in other countries. This calls for an extensive literature review for intensive care professionals.
Materials and methods. Using the data from 87 papers this review covers the composition, properties, methods of administration and delivery strategies of surfactant in the treatment and prevention of ARDS in patients with sepsis, severe complex injuries, inhalation injuries and a range of complications associated with thoracic and cardiovascular surgical procedures, massive blood transfusions, severe obstetric pathologies and the A/H1N1 pneumonia.
Results. The early administration of natural pulmonary surfactants within 24 hours following the onset of ARDS as a part of the ARDS combination treatment or prevention drives down the time on mechanical ventilation to six days or shorter, prevents ventilator-associated and hospital-acquired pneumonias, bringing the respiratory failure mortality rate down to 15–20%.
Discussion. Offering the first attempt to discuss the causes of failure of Phase III multicenter clinical trials outsideRussia andBelarus, this review outlines recent developments in synthetic and powdered pulmonary surfactant preparations.
Conclusion. Pulmonary surfactants are highly effective as a part of complex therapy in ARDS treatment and prevention, resulting in two to four fold drop in ARDS mortality rate. The timing of administration is seen as the key factor of the efficacy of surfactant therapy, explaining the differences in clinical trials results from different countries.

Glial tumors, and in particular anaplastic astrocytomas and glioblastoma multiforme (GBM), are aggressive brain tumors with poor prognosis and high recurrence rates. Current treatment strategies are based on open surgery, chemotherapy and radiation therapy. However, not a single one of these methods of treatment, alone or in combination, is effective in combating this disease, resulting in the average life expectancy following the diagnosis of under 15 months. Treatments are inefficient mainly due to the blood-brain barrier (BBB) that makes the delivery of drugs into the tumor mass difficult. With the development of nanotechnology the effectiveness of the drugs currently in use is on an increase and the reach to glial brain tumors is expanding. Nanoparticles are a preferred carrier of medicinal agents and dyes due to their size, availability of surface modification and the flexibility enabling the integration of several functional components into a single system. This makes it possible to direct the development of nanoparticles towards applications in the treatment and diagnosis of glial tumors. This dual approach helps to understand the location of the tumor tissue, bio-distribution of nanoparticles, and treatment progress and effectiveness. In order to improve the treatment and diagnosis approaches, various strategies can be applied to modify the surface of nanoparticles, including surface markers or so-called ligands and use the characteristics of the tumor microenvironment with specific targets which respond to specific stimuli. In this paper we review various strategies for the improvement of treatment and diagnosis of glial tumors, describe some surface markers and talk about opportunities for the introduction of nanoparticles into everyday clinical practice.
CLINICAL CASES

Introduction. An ectopic pancreas is an abnormality in which pancreatic tissue has grown outside its normal location with its own blood supply and ducts while having no anatomical, vascular or innervation connections with the pancreas situated normally. The accessory pancreas is the most frequent congenital disorder of this gland. The pancreatic tissue can be found in the walls of stomach, intestine, gallbladder, Meckel’s diverticulum, the liver, spleen and, seldom, in other organs having no contact with the pancreas. Currently the ectopic pancreas incidence is on the rise and amounts up to 0.2% on average in abdominal surgeries and is reported in 0.5–13% of autopsy cases. Most frequently the aberrant pancreas is located in the gastroduodenal zone (63–70% of all the heterotopic pancreas cases); most often it is found in the pylorus and antrum (85–95% of all the gastric ectopic pancreas cases).
Materials and methods. This paper presents a case of a successful treatment of a 39 year old male with an acute small intestinal obstruction caused by ectopic pancreatic tissue in the intestinal wall. The patient received a diagnostic laparoscopy and a mid-midline laparotomy with the wedge resection of the small intestine.
Results.The postoperative period was recorded as uneventful; the patient was discharged home on day nine following the surgery after removal of cutaneous sutures. The pathology of the small intestinal fragment with the polyp-like neoplasm identified heterotypic pancreatic foci (with acini and ducts) located between muscular bands, with extensive areas of haemorrhaging and necrosis.
Conclusion.The diagnosis of the ectopic pancreas tissue in intestinal wall is an extremely complex issue in abdominal surgery; this diagnosis is normally made only when complications occur. Pathomorphological verification is of paramount importance to make the final diagnosis of this disease, making it possible to identify correctly the cause and mechanism of the development of an acute surgical disorder.
LABORATORY AND EXPERIMENTAL INVESTIGATION
A number of questions arise when choosing methods for experiments related to next-generation sequencing. On the one hand, while working with RNA extraction, added reagents and their residues can often inhibit sensitive chemicals with which the sequential synthesis is carried out for the sequencing. On the other hand, processing the same data using different software for the analysis can also impact on the sequencing results. This paper will present the step by step procedure for the preparation of samples taken from human biological fluids for subsequent sequencing of small RNAs, small noncoding RNAs in particular. Regarding the methods of extraction or isolation of RNAs, we found that low RNA yield can be improved significantly by following the isolation method for total RNA and its fractions included in Ambion’s MirVana PARIS kit, but only if using a special approach and modifying the organic extraction step. Compared to others, the methods supplied with commercially available kits at the time of researching this paper require only one organic extraction. This simple but, as it turned out, very useful modification makes it possible to access previously unavailable material. Potential advantages of this modification include a more complete profiling of small non-coding RNAs and a broader access to small sample volumes, as a rule, access to human biological fluids which can be prepared for RNA sequencing on the Illumina platform.
BRIEF COMMUNICATIONS


ISSN 2307-0501 (Online)





























