


ORIGINAL ARTICLES
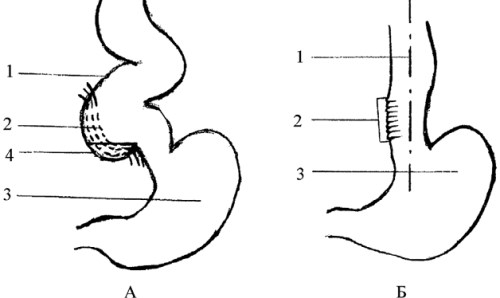
Introduction. Stage IV (sigmoid) cardia achalasia (CA) is characterized by marked esophageal dilation and S-shaped deformity, leading to severe impairment of bolus transit and significant deterioration in quality of life. In end-stage disease, conventional Heller–Gottstein myotomy often fails to restore adequate esophageal emptying, and esophagectomy is frequently considered despite its substantial morbidity. In recent years, interest has grown in organ-preserving procedures that include correction of axial esophageal deformity. Aim: this study aimed to compare outcomes of the Heller–Gottstein procedure in patients with stage IV CA using the classical technique versus a modified approach incorporating straightening of the vertical esophageal axis.
Materials and methods. A comparative analysis was performed in 63 patients with stage IV CA who underwent surgery before and after adoption of the modified technique. Group I included patients treated between 1982 and 2007 with classical Heller–Gottstein myotomy. Group II included patients operated on between 2008 and 2024 using the modified approach with vertical axis correction. Treatment efficacy was assessed in the early postoperative period and at 24 months using clinical evaluation, endoscopy, radiography, the Eckardt score, and the Gastrointestinal Quality of Life Index (GIQLI).
Results. The groups were comparable preoperatively across key baseline characteristics (p > 0.05). Persistent dysphagia resolved in all patients in the early postoperative period. However, S-shaped deformity persisted in 100% of Group I and in 21.4% of Group II (p < 0.001). At 24 months, Group II demonstrated significantly lower symptom severity according to the Eckardt score (2 [0–2.25] vs 3 [1–4], p = 0.044), a markedly lower rate of persistent sigmoid deformity (5% vs 71.4%, p < 0.001), and higher GIQLI scores (133 vs 114 points, p = 0.001).
Discussion. Correction of the vertical esophageal axis appears to be a key determinant of improved long-term functional outcomes in stage IV CA. Conclusion. The incorporation of vertical axis straightening into the Heller–Gottstein myotomy significantly improves long-term functional results in patients with stage IV cardia achalasia.
Introduction. In Russia, 72.5% of newly diagnosed breast cancer (BC) cases are detected at early stages. Nodal status remains a key factor in determining the extent of surgical treatment. Although sentinel lymph node biopsy (SLNB) is the standard staging procedure for cN0 disease, large prospective trials have demonstrated that SLNB can be safely omitted in selected patients with cT1–2N0 tumors.
Aim. This study aims to evaluate long-term oncologic outcomes and quality-of-life parameters in patients with cT1–2cN0 breast cancer according to the extent of axillary surgery.
Materials and methods. This study included 204 patients with luminal subtypes of primary operable breast cancer treated at the P. Hertsen Moscow Oncology Research Institute (MORI) between 2017 and 2022. Patients were assigned to two groups: SLNB omitted (Group I, n = 51) and SLNB performed (Group II, n = 153). Allocation was carried out using pseudorandomization in a 1:3 ratio stratified by clinical and morphologic tumor characteristics. The mean patient age was 58.1 years. Quality of life was assessed using the EORTC QLQ-BR23 questionnaire during the first postoperative year.
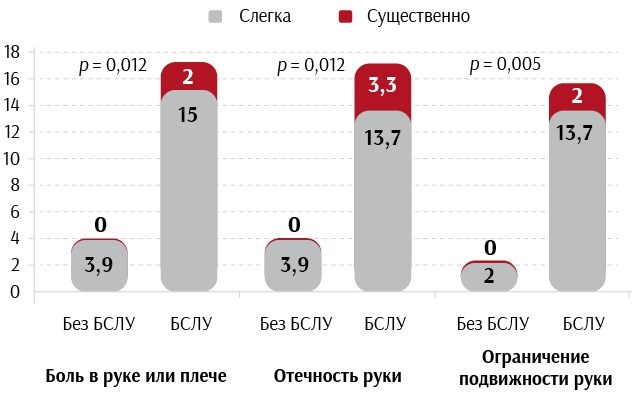
Results. The median follow-up was 76.8 months. Disease progression occurred in 4.4% of patients. Regional recurrences were observed in 1.5% of cases, and distant metastases in 2.5%. Median progression-free survival and overall survival were not reached. Five-year overall survival was 100%. Recurrence-free survival was 95.2 ± 3.4% in Group I and 98.0 ± 1.1% in Group II (p > 0.05). Shoulder and arm symptoms during the first year were reported by 4% and 17% of patients, respectively (p = 0.012). Discussion. Our findings are consistent with international evidence: in patients with cT1–2cN0 luminal breast cancer, SLNB can be safely omitted without compromising oncologic outcomes. Avoiding axillary lymph node dissection is associated with lower rates of lymphedema, pain, and reduced arm mobility, thereby improving quality of life. Multicenter studies support the trend toward de-escalation of axillary surgery while maintaining survival outcomes.
Conclusion. Patients with cT1–2cN0 luminal breast cancer may be considered candidates for omission of SLNB without loss of oncologic efficacy.
REVIEWS
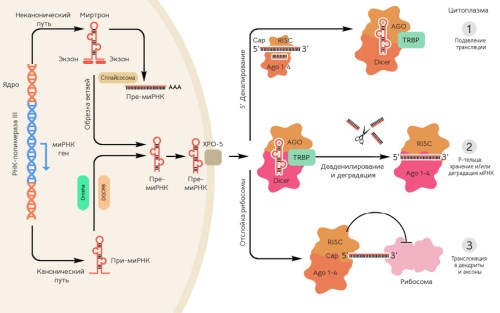
Extracellular vesicles (EVs), such as exosomes and microvesicles (MVs), are lipid bilayer-enclosed nanoparticles released by various cells. Their diameters range from 30 nm to several micrometers, and they carry biological cargo, including proteins, lipids, RNA, and DNA, for local and distant intercellular communication. EVs play important role in the development and progression of numerous human diseases, including cancer. EVs are considered promising candidates for clinical applications as carriers of therapeutic agents and as diagnostic tools, owing to their capacity to cross biological barriers, such as the blood-brain barrier (BBB), and target specific cells. The visualization of EVs is essential to understand their roles, from packaging genetic material and signaling molecules during their biogenesis in donor cells to tracking uptake by recipient cells and downstream signaling following internalization. The clinical translation of EVs in diagnostics and therapy remains limited by challenges associated with their high-resolution visualization both in vitro and in vivo, primarily due to their small size. Researchers worldwide are developing innovative labeling and visualization strategies to unlock EV full potential. This review covers current and emerging EV visualization approaches in research settings and discusses the advantages and limitations of the major imaging strategies.
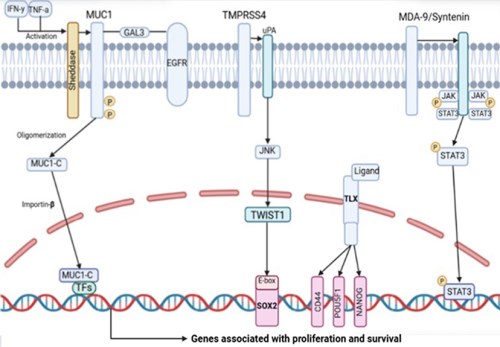
Prostate cancer (PCa) remains one of the most prevalent malignancies in men and a leading cause of cancer-related mortality, particularly in its castration-resistant and metastatic forms. Accumulating evidence highlights the central role of cancer stem cells (CSCs) in tumor initiation, progression, intratumoral heterogeneity, and the resistance to therapy and radiation. This review summarizes current data and provides an in-depth analysis of four promossing regulators of CSC-associated stemness and cellular plasticity: the oncoprotein MUC1-C, the type II transmembrane serine protease TMPRSS4, the orphan nuclear receptor TLX, and the PDZ-domain adaptor protein MDA-9/Syntenin. For each molecule, we discuss structural features, expression patterns in prostate tissue, and involvement in key oncogenic signaling pathways, including Wnt/β-catenin, PI3K/AKT, MAPK, STAT3, NOTCH, and TGF-β. Their contributions to epithelial-mesenchymal transition (EMT), maintenance of the CSC phenotype, androgen-independent growth, and resistance to standard therapies are examined in detail. Particular emphasis is placed on in vitro and in vivo evidence demonstrating the significance of MUC1-C, TMPRSS4, TLX, and MDA-9/syntenin as biomarkers of aggressive PCa and as targets for precision therapeutics and immunotherapy.
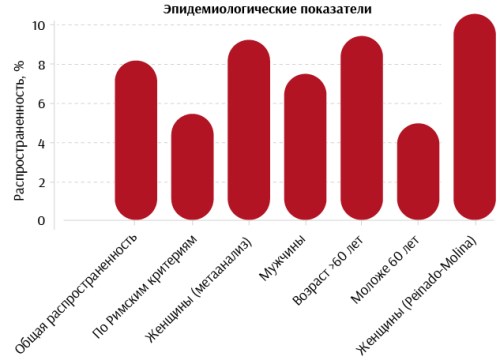
Anal sphincter insufficiency (ASI) is a prevalent condition that leads to fecal incontinence (FI) and a substantial decline in health-related quality of life. Literature reports an average ASI prevalence of 8% among adults, underscoring its significance as both a medical and social issue that requires improved diagnostic and therapeutic strategies. Conservative management, including pelvic floor muscle training, biofeedback therapy, and dietary modification, often provides only limited and temporary benefit. When conservative measures fail, minimally invasive procedures and, subsequently, surgical interventions are considered. However, even surgical approaches carry a substantial long-term recurrence risk. Regenerative medicine, particularly the use of stem cells as a primary or adjunctive therapeutic modality, has generated substantial interest. Studies show that adipose-derived mesenchymal stem cells (AD-MSCs) improve sphincter morphology and promote restoration of muscle fibers without direct differentiation into smooth muscle. Bone-marrow-derived mesenchymal stem cells (BM-MSCs) demonstrate similar effects, acting through paracrine signaling and immunomodulation to enhance muscle morphology and contractility. In contrast, the therapeutic potential of induced pluripotent stem cells (iPSCs) remains largely unexplored. At present, the evidence base for all stem-cell therapies remains limited, with no standardized treatment protocols being established. Robust confirmation of efficacy requires multicenter randomized trials. This review summarizes current data on ASI treatment and identifies priority directions for future research in regenerative medicine aimed at managing this condition.

Arterial upper gastrointestinal bleeding (UGIB) remains a major clinical challenge due to high rates of rebleeding even after technically successful endoscopic hemostasis. A systematic analysis of 60 contemporary publications shows that transcatheter arterial embolization (TAE) has evolved from a rescue intervention into an integral component of multidisciplinary strategies aimed at achieving durable hemostasis. Indications and contraindications for endovascular treatment are summarized, and an algorithm for embolic agent selection is proposed based on vessel caliber, anatomic variability, and pathologic remodeling of the celiac and mesenteric arterial systems. Prophylactic embolization in patients who achieve primary endoscopic hemostasis but meet high-risk criteria for rebleeding significantly reduces recurrent hemorrhage and in-hospital mortality compared with endoscopic therapy alone. In cases of refractory bleeding, TAE demonstrates high clinical efficacy and offers an organ-preserving alternative to surgery, particularly in patients with elevated operative risk. The accumulated evidence supports the incorporation of preventive embolization into clinical protocols for this patient population.
Thyroid cancer is one of the most common endocrine malignancies worldwide. Surgical resection remains the standard care; however, minimally invasive approaches are increasingly being investigated for patients with low-risk cases, particularly papillary thyroid microcarcinoma (PTMC). This review summarizes current evidence on the use of radiofrequency ablation (RFA) in the management of differentiated thyroid carcinoma, with a primary focus on papillary thyroid carcinoma. 27 key publications were analyzed, including international guidelines, meta-analyses, and prospective and retrospective studies. Available data indicate that RFA achieves local tumor control and recurrence-free survival rates comparable to those of surgical management in appropriately selected low-risk patients, while significantly reducing procedure-related morbidity and preserving thyroid function. The technique demonstrates particular efficacy in patients with solitary tumors of up to 1 cm (T1aN0M0) without evidence of metastasis. This review provides a comprehensive evaluation of accumulated clinical data, direct comparison between RFA and thyroid surgery, and an analysis of long-term outcomes as reflected in major guidelines from 2022–2025. Current evidence suggests that RFA represents an emerging organ-preserving strategy that maintains oncologic efficacy in low-risk papillary thyroid carcinoma. Further randomized trials are required to define its role within standardized treatment algorithms.
Lower extremity peripheral artery disease (PAD) remains a major medical and social challenge due to its elevated cardiovascular risk and substantial reduction in patient quality of life. This review synthesizes contemporary literature, clinical guidelines, and our own clinical observations. 66 publications were analyzed, predominantly from the past decade, with earlier sources included when they provided foundational or high-value evidence. PAD pathogenesis involves hemostatic disturbances, including platelet activation, endothelial dysfunction, and hypercoagulability, which drive atherosclerosis progression and tissue ischemia. Pharmacological correction of hemostatic abnormalities remains the cornerstone of treatment and prevention of PAD-related complications. Modern clinical trials support an integrated management strategy combining pharmacotherapy, risk-factor control, and lifestyle modification to improve prognosis and quality of life. Future research directions include the development of agents targeting inflammatory pathways and endothelial function, as well as personalized therapeutic approaches based on individual hemostatic profiles and comorbidities. A deeper understanding of the role of the coagulation system in PAD pathogenesis, together with the application of modern pharmacological approaches, may optimize treatment outcomes and reduce the overall disease burden at the population level.
CLINICAL CASES
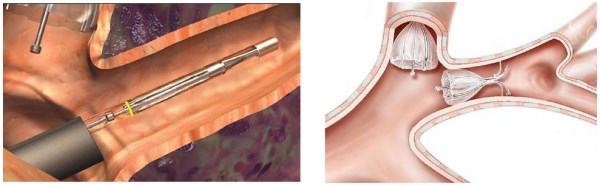
Introduction. Endoscopic lung volume reduction (ELVR) with endobronchial valves is a minimally invasive technique used in severe emphysema-dominant chronic obstructive pulmonary disease (COPD). The procedure improves respiratory mechanics and reduces dyspnea by inducing atelectasis in hyperinflated lung segments without thoracotomy. ELVR is applied as palliative therapy or as a bridge to lung transplantation and can substantially improve quality of life in carefully selected patients. Segmental endobronchial valve therapy is now an established option for lung volume reduction in patients with upper-lobe-predominant emphysema and limited exercise tolerance.
Materials and methods. Case report. A 73-year-old patient with COPD, heterogeneous non-bullous emphysema, with severe upper-lobe predominance in the right lung, and grade 2 cor pulmonale had experienced multiple hospitalizations. ELVR was performed by placing endobronchial valves to achieve bronchial blockade of the right upper-lobe segments.
Results and discussion. The therapeutic effect of endobronchial valve therapy in COPD is achieved by restricting airflow to severely emphysematous regions. In this patient, segmental blockade of the right upper lobe reduced the severity of respiratory insufficiency and produced a meaningful improvement in quality of life.
Conclusion. Bronchoscopic lung-volume reduction with endobronchial valves is an effective approach for improving pulmonary function and exercise capacity in patients with severe COPD and upper-lobe-predominant emphysema.
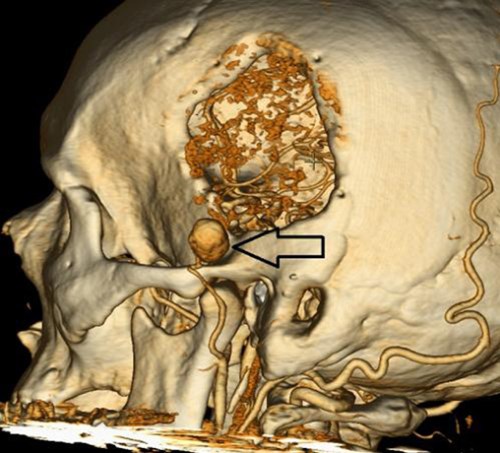
Introduction. This article presents a rare vascular complication that developed after cranioplasty. Aim. This study aims to describe the successful surgical treatment of a superficial temporal artery (STA) aneurysm that arose as a complication of cranioplasty.
Materials and methods. A 60-year-old patient developed a painful, pulsatile 5-cm STA aneurysm one month after evacuation of an intracerebral hematoma followed by cranioplasty. The diagnosis was confirmed by computed tomography angiography (CTA). Emergency open aneurysmectomy was performed under endotracheal anesthesia, with arterial ligation and resection of the aneurysmal sac.
Results and discussion. The postoperative course was uneventful, and the patient was discharged on postoperative day 7. Aneurysm formation was attributed to intraoperative arterial injury during the preceding procedure. This complication is exceedingly rare. Severe pain and the risk of rupture constituted clear indications for urgent open surgery, despite the theoretical feasibility of endovascular treatment.
Conclusion. Open surgical resection of a superficial temporal artery aneurysm proved to be an effective and safe treatment for this rare complication of cranioplasty.
Introduction. Pulmonary carcinoid tumors are rare neuroendocrine neoplasms characterized by a relatively favorable clinical course. Surgical resection remains the primary treatment for typical carcinoid, with preference given to lung-preserving procedures, particularly bronchoplastic resections.
Materials and methods. This report presents a clinical case of successful minimally invasive surgical treatment in a 72-year-old woman with a typical carcinoid of the right main bronchus.
Results and discussion. Thoracoscopic isolated resection of the right main and intermediate bronchi was performed with reconstruction using a polybronchial anastomosis while preserving the interlobar spur between the upper lobar and intermediate bronchi. The procedure proved highly effective. An R0 resection was achieved and confirmed by intraoperative frozen-section analysis. No postoperative complications occurred. Long-term follow-up demonstrated no evidence of recurrence, with preservation of satisfactory pulmonary function.
Conclusion. This case demonstrates the feasibility and oncologic adequacy of minimally invasive bronchoplastic procedures as an alternative to more extensive pulmonary resections in patients with centrally located typical carcinoid tumors.
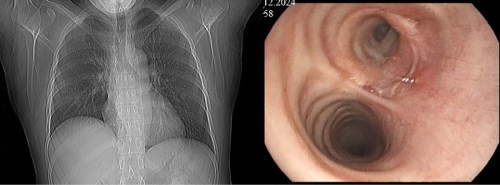
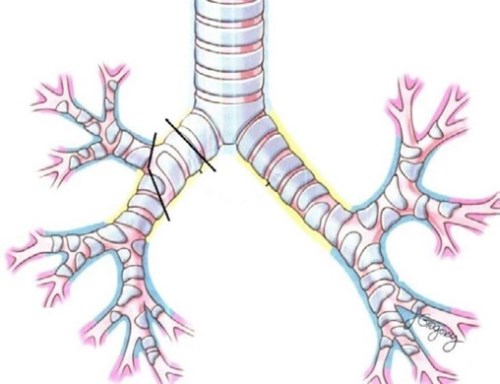
Introduction. Although traumatic injuries of the tracheobronchial tree are rare, they are potentially life-threatening conditions that require early recognition and prompt surgical management. Diagnosis is frequently delayed due to subtle clinical manifestations that are often obscured by associated injuries. Up to 80% of patients die before reaching the hospital. Most injuries involve the right main bronchus and are located within 2 cm of the carina, reflecting its anatomic vulnerability. Mortality is highest in patients with bilateral bronchial injuries.
Materials and methods. We report a 34-year-old woman who sustained complete avulsion of the right main bronchus after a motor vehicle accident. The injury went unrecognized during the acute phase. One month later, bronchial atresia developed acompanied by purulent secretion and dyspnea. Delayed bronchoplastic reconstruction was performed, consisting of right upper lobectomy and end-to-end anastomosis between the right main bronchus and the bronchus intermedius. The procedure was uneventful, and the patient was discharged on postoperative day 8 without complications. Follow-up bronchoscopy at 1.5 months confirmed patent anastomosis. Contrast-enhanced computed tomography demonstrated restoration of aeration of the right lung.
Results and discussion. Tracheobronchial injuries remain uncommon yet life-threatening conditions that demand prompt diagnosis and timely surgical intervention. Main bronchial rupture in closed chest trauma typically results from combined thoracic compression and acute intrabronchial pressure rise against a closed glottis. Delayed diagnosis may lead to irreversible parenchymal damage and necessitate radical resection. Timely bronchoplastic reconstruction preserves pulmonary function, allowing pneumonectomy to be avoided.
Conclusion. This case demonstrates that successful surgical management is feasible even in the delayed post-traumatic period, provided that viable lung parenchyma is preserved and thorough preoperative assessment is performed.

ISSN 2307-0501 (Online)





























